

Background: The skull is partially created and composed of numerous sutures. During development the skull is composed of six separate cranial bones which are held together by sutures which are made up of fibrous and elastic tissue. These sutures keep the skull bones separate for up to 18 months after birth to allow for brain growth at which point they grew together and remain so through adulthood.
One of these cranial sutures and the only one located directly in the midline is the sagittal suture. It is the suture that connects the two parietal bones. It is the cranial suture that takes the longest to close often not completely so until around thirty years of age. Early closure of this suture in infancy creates the classic scaphocephaly craniosynostosis with severe head shape aberration. But much less severe forms of scaphcephaly do occur and are noted by a prominent sagittal ridge or sagittal crest = from the bregma anteriorly back to the vertex posteriorly. This can be accompanied by a relative parasagittal deficiency which can magnify the appearance of the sagittal crest.
While the sagittal crest can be burred down there are limits as to how much it can be reduced. The thickness of the sagittal crest is often not greater than 6 or 7mms thick before the inner bony table is encountered or breached. In some patients the sagittal crest may be thicker but it is not assured. Thus maximal sagittal crest reduction may not make the top of the head acquire a convex shape, only blunting of sagittal point.
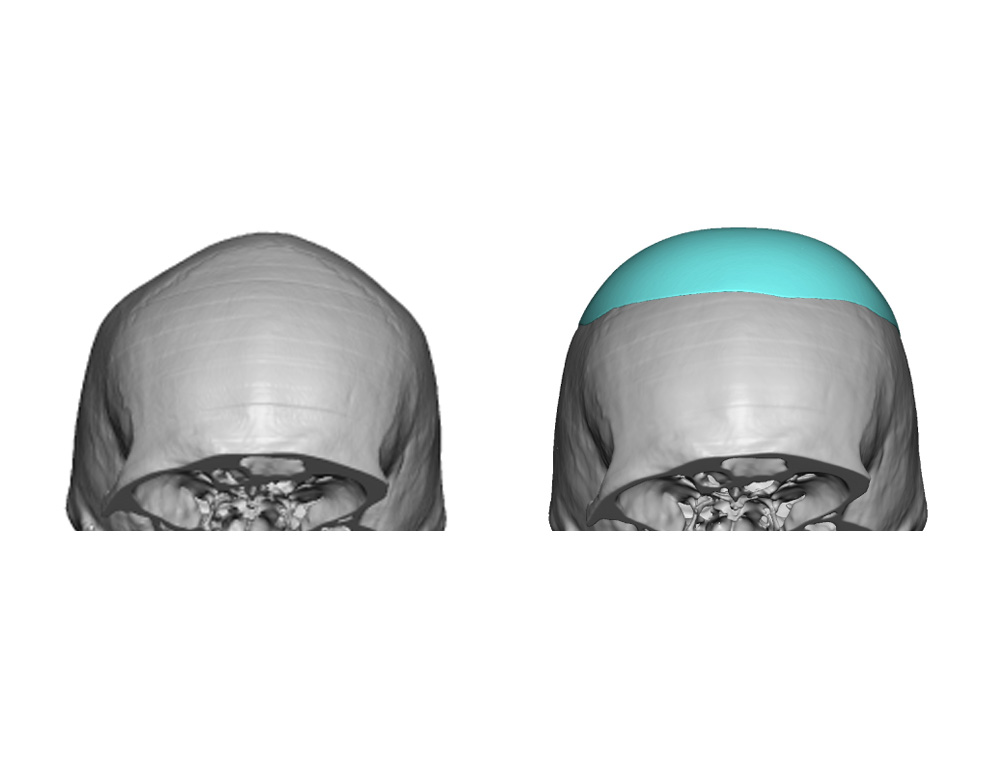
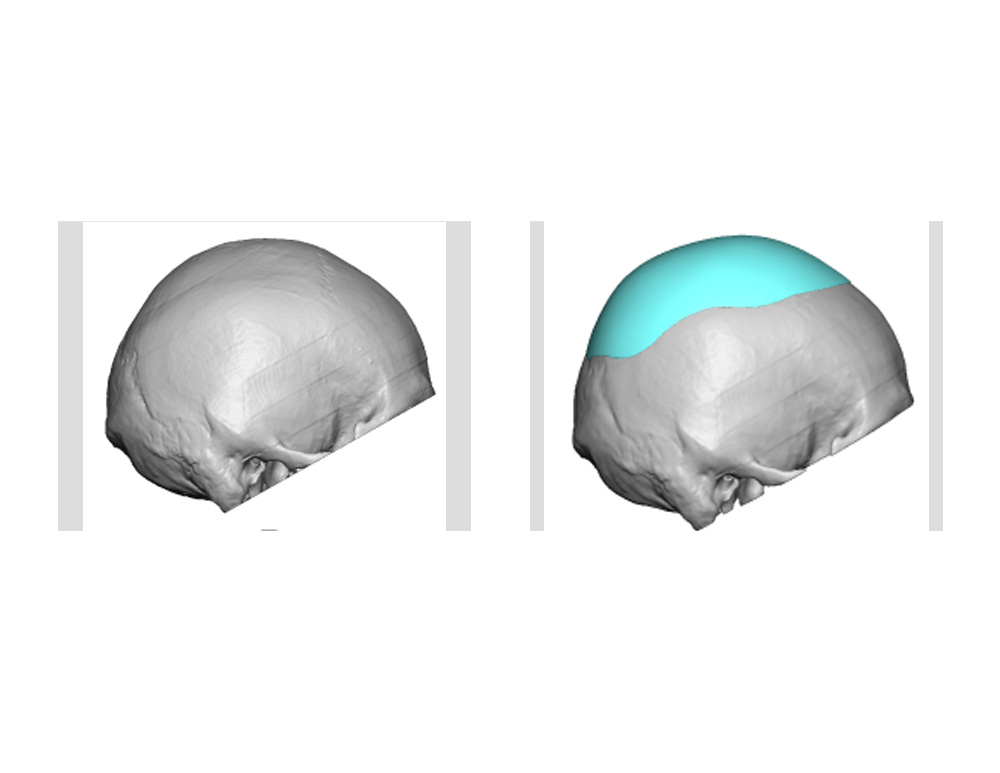 Case Study: This 35 year-old male wanted to change the shape of the top of his head. It had a very triangular shape, almost to the point of an inverted V shape. There was a prominent sagittal crest but also a relative parasagittal deficiency. It was felt that sagittal crest reduction alone would not provide much improvement. Instead, recontouring of the top of the skull was elected to be done with a custom designed skull cap implant made from the patient’s 3D CT scan.
Case Study: This 35 year-old male wanted to change the shape of the top of his head. It had a very triangular shape, almost to the point of an inverted V shape. There was a prominent sagittal crest but also a relative parasagittal deficiency. It was felt that sagittal crest reduction alone would not provide much improvement. Instead, recontouring of the top of the skull was elected to be done with a custom designed skull cap implant made from the patient’s 3D CT scan.
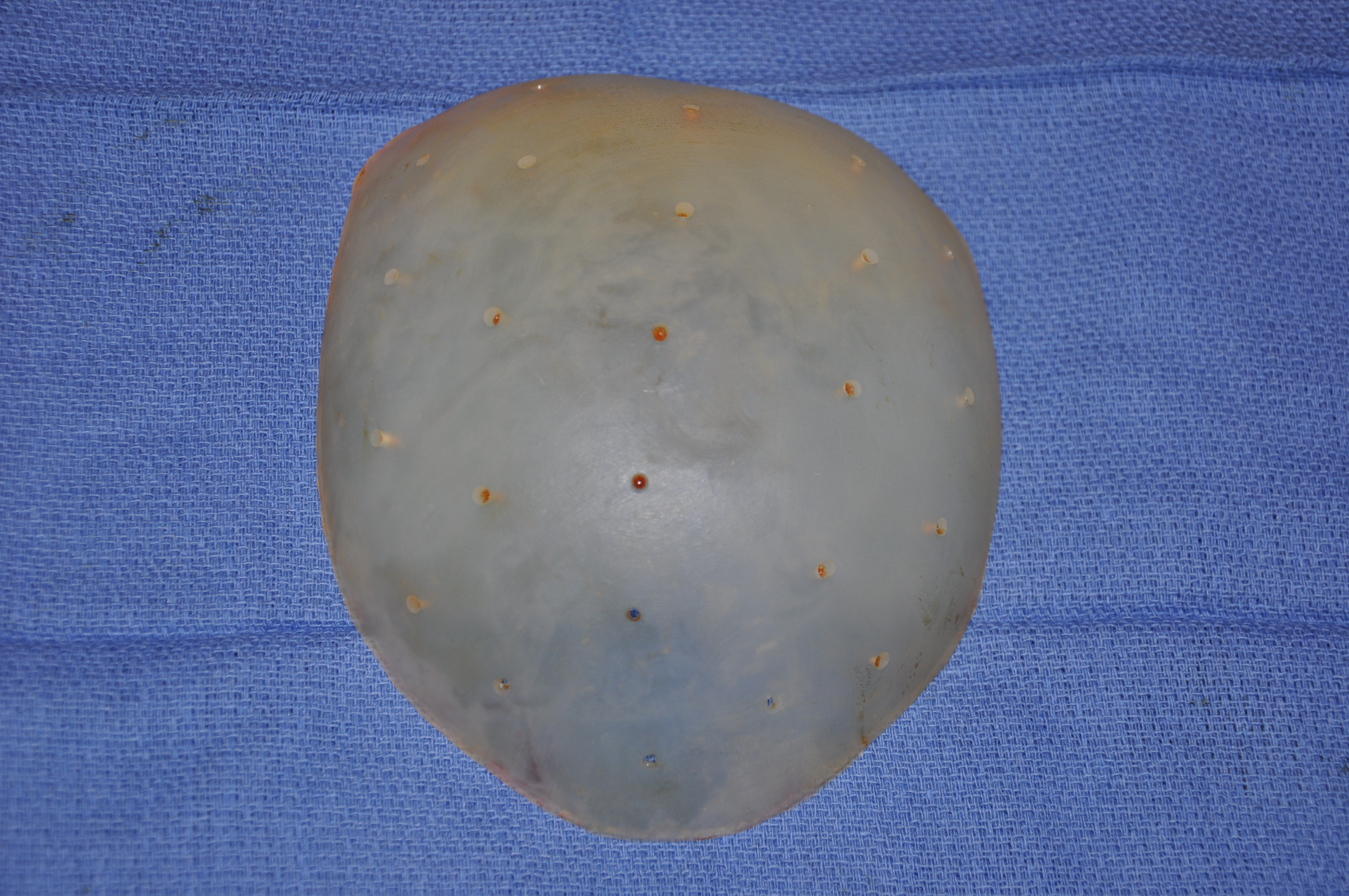 Under general anesthesia a 9cm scalp incision was made perpendicular to the sagittal crest just anterior to the vertex. Wide subperiosteal undermining was done to develop the implant pocket. Prior to insertion the skull cap implant had multiple perforation holes placed through its thickness with a 3mm dermal punch. The implant was inserted and secured down to the bone with a single 1.5mm titanium screw. A drain was placed to be removed the next day.
Under general anesthesia a 9cm scalp incision was made perpendicular to the sagittal crest just anterior to the vertex. Wide subperiosteal undermining was done to develop the implant pocket. Prior to insertion the skull cap implant had multiple perforation holes placed through its thickness with a 3mm dermal punch. The implant was inserted and secured down to the bone with a single 1.5mm titanium screw. A drain was placed to be removed the next day.

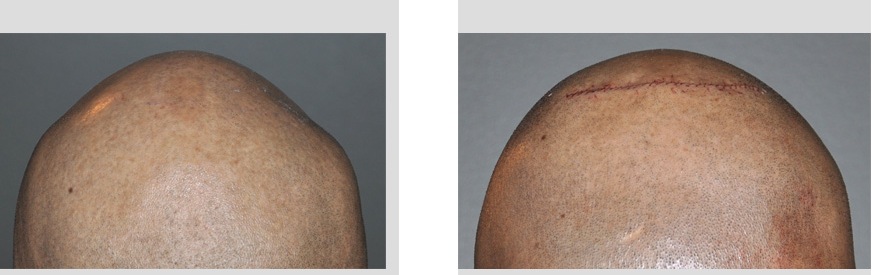 The change in the shape of the skull was both immediate and significant. The upper head shape was convex and no longer pointed as can be seen from both the front and back views. It should be noted that this was just one day after surgery so swelling may make the height of the head higher than it may eventually be. But clearly the head shape reflets what the shape of the designed implant was. It will take months to eventually determine how smooth and indiscernible the transition from the implant edges to the bone. (which should be smooth and non-visible)
The change in the shape of the skull was both immediate and significant. The upper head shape was convex and no longer pointed as can be seen from both the front and back views. It should be noted that this was just one day after surgery so swelling may make the height of the head higher than it may eventually be. But clearly the head shape reflets what the shape of the designed implant was. It will take months to eventually determine how smooth and indiscernible the transition from the implant edges to the bone. (which should be smooth and non-visible)
The custom skull implant provides a very effective solution for the sagittal crest skull deformity that has associated parasagittal deficiencies. The thickness of the implant over the sagittal crest only needs to be very thin (1mm) while the parasagittal area is much thicker as it blends to a fine edge into the upper temporal region.
Highlights:
1) The sagittal ridge skull deformity is the result of sagittal suture overgrowth, parasagittal deficiency or a combination of both.
2) Parasagittal augmentation can recontour the top of the head to make it more convex rather than triangular in shape.
3) A custom skull implant offers the most assured method of top of the head reshaping with the smallest incision to do so.
Dr. Barry Eppley
Indianapolis, Indiana