

Background: Skull defects occur in children for a variety of reasons. But one of the most common causes is early surgery for congenital skull deformities. When reshaping large portions of the skull their complete healing depends on the natural osteogenic capability of the underlying dura. This is usually very robust at very young ages but fades quickly after the first few years of life.
Reconstructing skull defects in children can be done by several techniques. One method is to use the patient’s own bone to do so. This is the most logical approach but its disadvantages is that one has to create another skull defect site and such bone does not always heal smoothly. The next option would be to use allogeneic or cadaver bone grafts. This saves a donor site but does not get around how smoothly, or non-smoothly, the resultant skull contour will be.
The third skull contouring material is that of hydroxyapatite cements. These synthetic calcium phosphate materials have a long history of use in craniofacial surgery for skull defect and contouring reconstructions. They are less well known for use in children but their value in these pediatric skull applications is no less significant.
Case Study: This 9 month-old infant male cild initially underwent reconstruction for a unilateral coronal craniosynostosis condition. The surgery was performed using supraorbital bar reshaping as well as a barrel-stave technique to expand out the overlying forehead bone.He went on well and when seen years later at age 8 he had a slight flattening of the lateral forehead and a palpable full-thickness bone defect along the original coronal suture line.
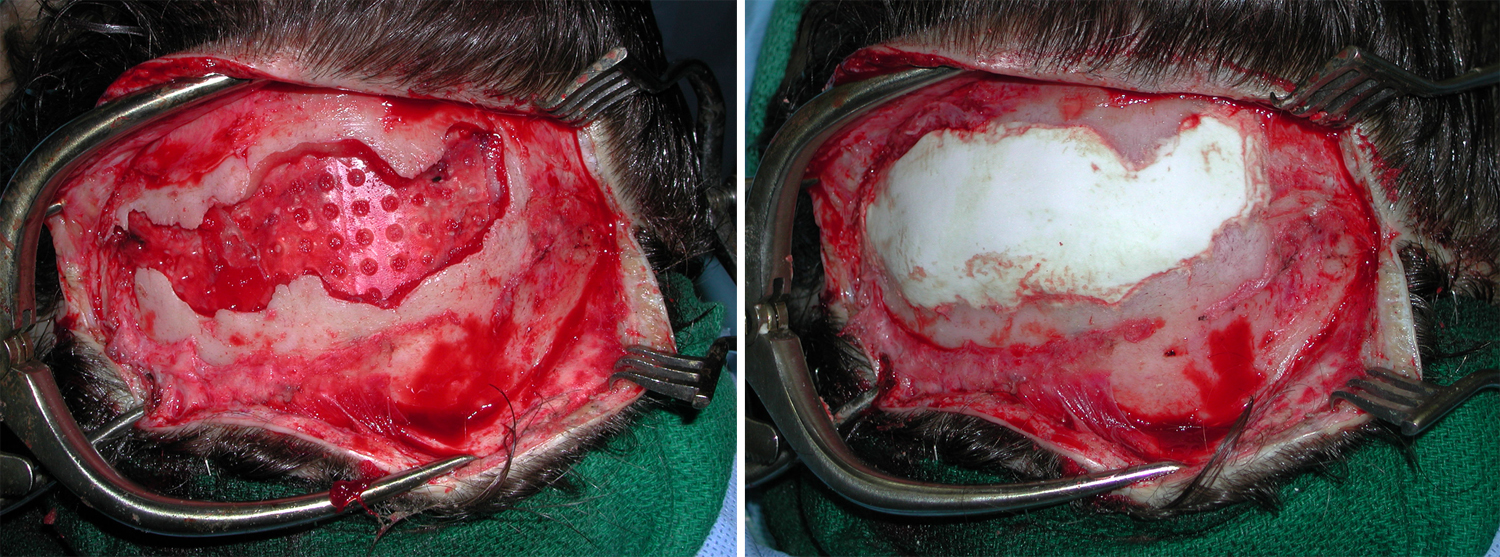
 Under general anesthesia and through his existing coronal scalp incision, the bone defect along the original coronal suture line was exposed. The dura was elevated off of the bone edges entirely around the defect. A Lactosorb mesh plate (resorbable PLLA-PGA) was placed on the underside of the bone and cut to lock in between the dura and the bone edges. Hydroxyapatite cement was applied into the bone defect using the mesh plate as its backing. It was then contoured to be flush with the surrounding skull contours and allowed to set.
Under general anesthesia and through his existing coronal scalp incision, the bone defect along the original coronal suture line was exposed. The dura was elevated off of the bone edges entirely around the defect. A Lactosorb mesh plate (resorbable PLLA-PGA) was placed on the underside of the bone and cut to lock in between the dura and the bone edges. Hydroxyapatite cement was applied into the bone defect using the mesh plate as its backing. It was then contoured to be flush with the surrounding skull contours and allowed to set.
Hydroxyapatite cement can be used to both fill in skull defects as well as can be placed as an onlay augmentation material. While more extensively used in adults, it can be just as effectively used in children. There is always the question of what happens to the bone cement as the skull continues to grow. My observation is that the skull bone on top and underneath it and it simply gets pushed out jus like normal skull bone with dow with ongoing appositional skull growth.
Highlights:
- Skull defects in children can be treated by either bone grafts or hydroxyapatite cement.
- When using bone cements in a full-thickness skull defect, a floor against the dura must be created to support the material.
- Bone cements offer a facile material to fill and contour skull defects.
Dr. Barry Eppley
Indianapolis, Indiana