

Background: The shape of the top of the head is highly influenced by the development and growth of the sagittal suture. This cranial suture lies between the anterior and posterior fontanelles (soft spots) that are present at birth and close shortly thereafter. Premature fusion of the entire sagittal suture produces a well known congenital skull defect known as craniosynostosis with an abnormally long and narrow skull shape that requires early surgery for correction.
But there are a variety of much smaller forms of sagittal suture abnormalities which produce a variety of raised midline ridges on the top of the head. Between the original posterior and anterior fontanelles the sagittal ridge can become thickened and sit higher than the surrounding bone. In some cases it is an isolated raised ridge of bone. But in other cases the raised sagittal crest is accompanied by a corresponding deficiency of the surrounding bone. Put together this creates a very peaked skull shape like that of a roof.
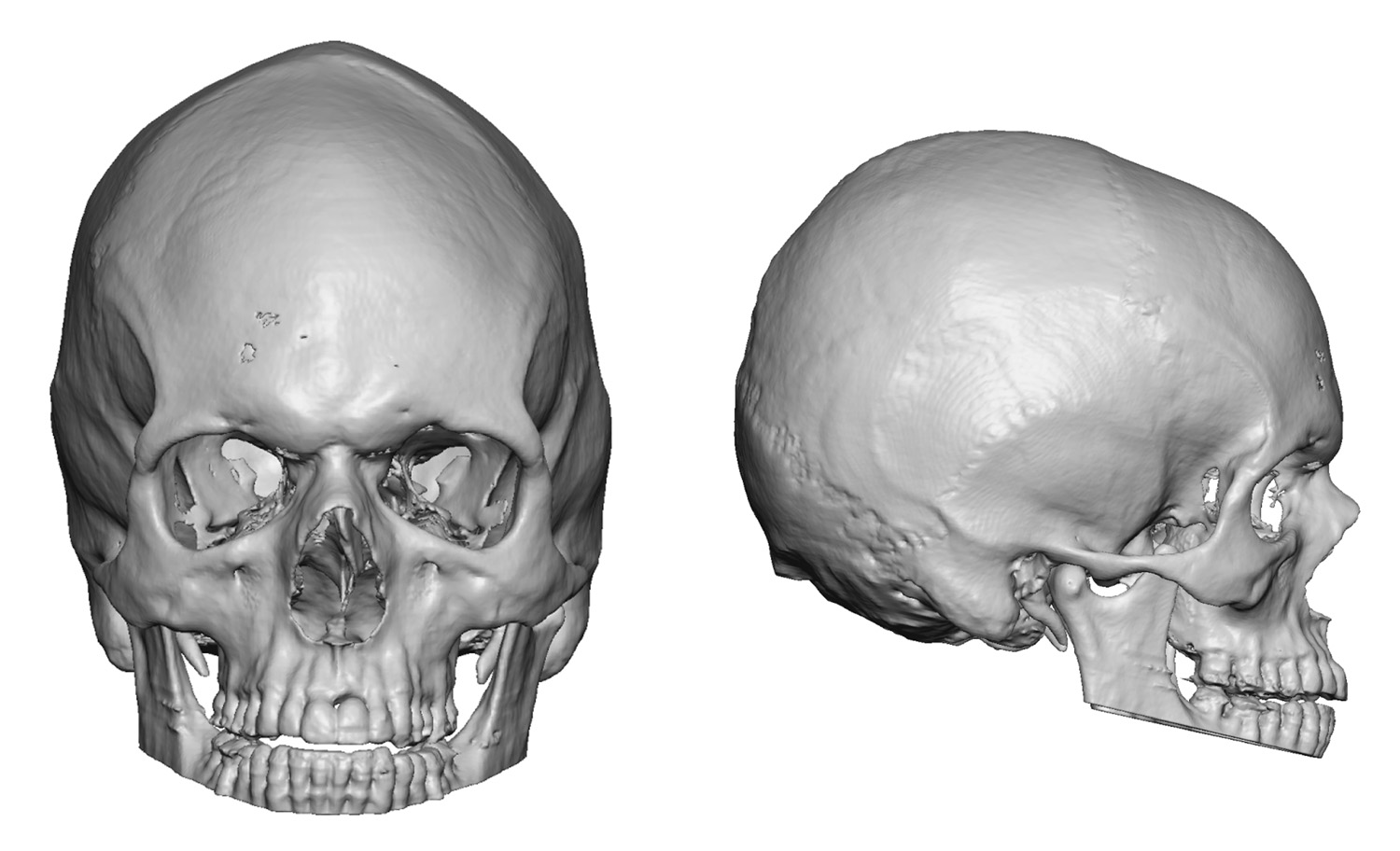
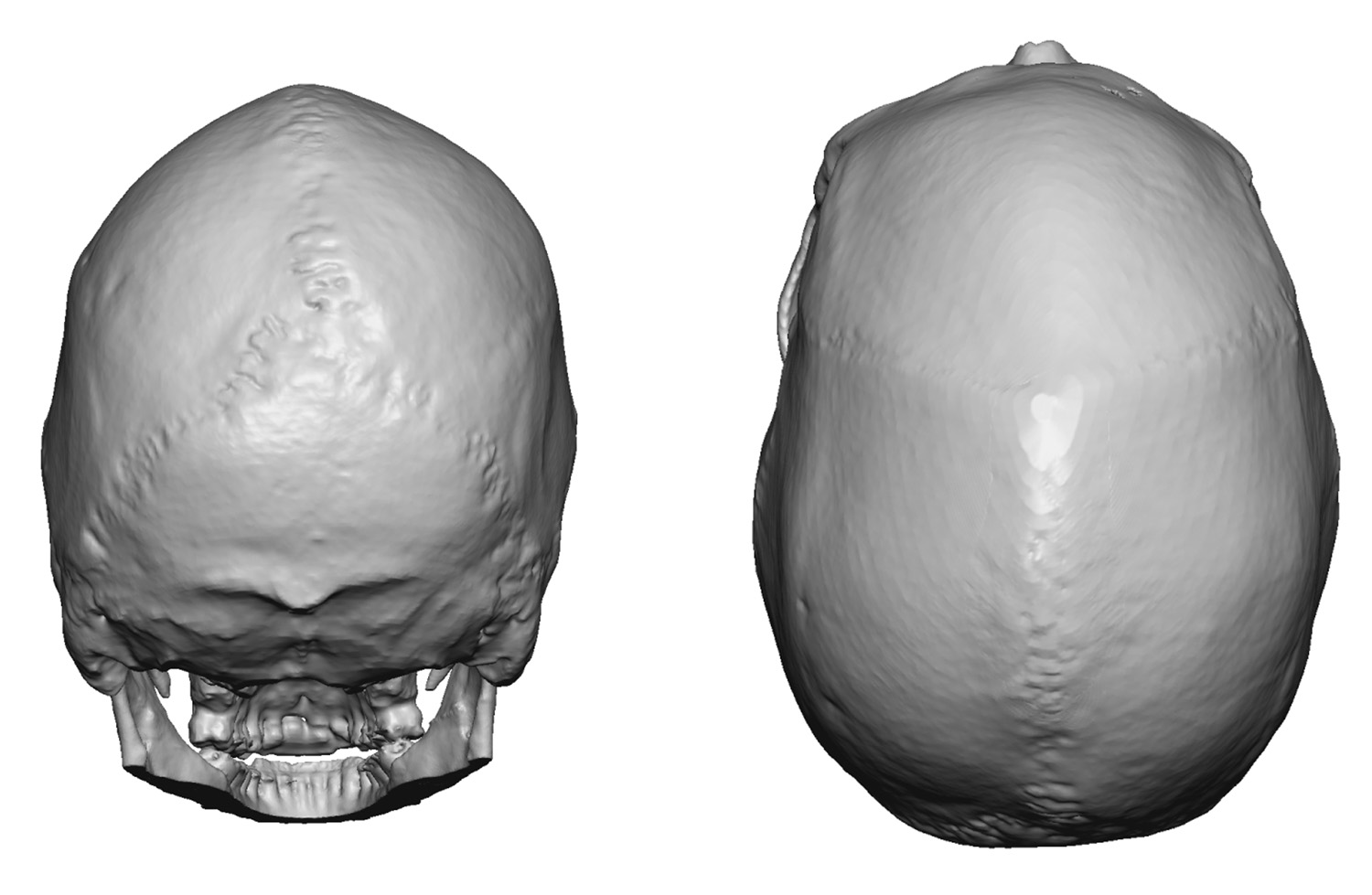 Case Study: This 50 year-old male was bothered by a skull shape that was becoming apparent as his hair was thinning. He described it as a high sagittal ridge with both sides sloping away from the middle. This gave the top of his head a more triangular shape. This was confirmed by a 3D CT scan.
Case Study: This 50 year-old male was bothered by a skull shape that was becoming apparent as his hair was thinning. He described it as a high sagittal ridge with both sides sloping away from the middle. This gave the top of his head a more triangular shape. This was confirmed by a 3D CT scan.
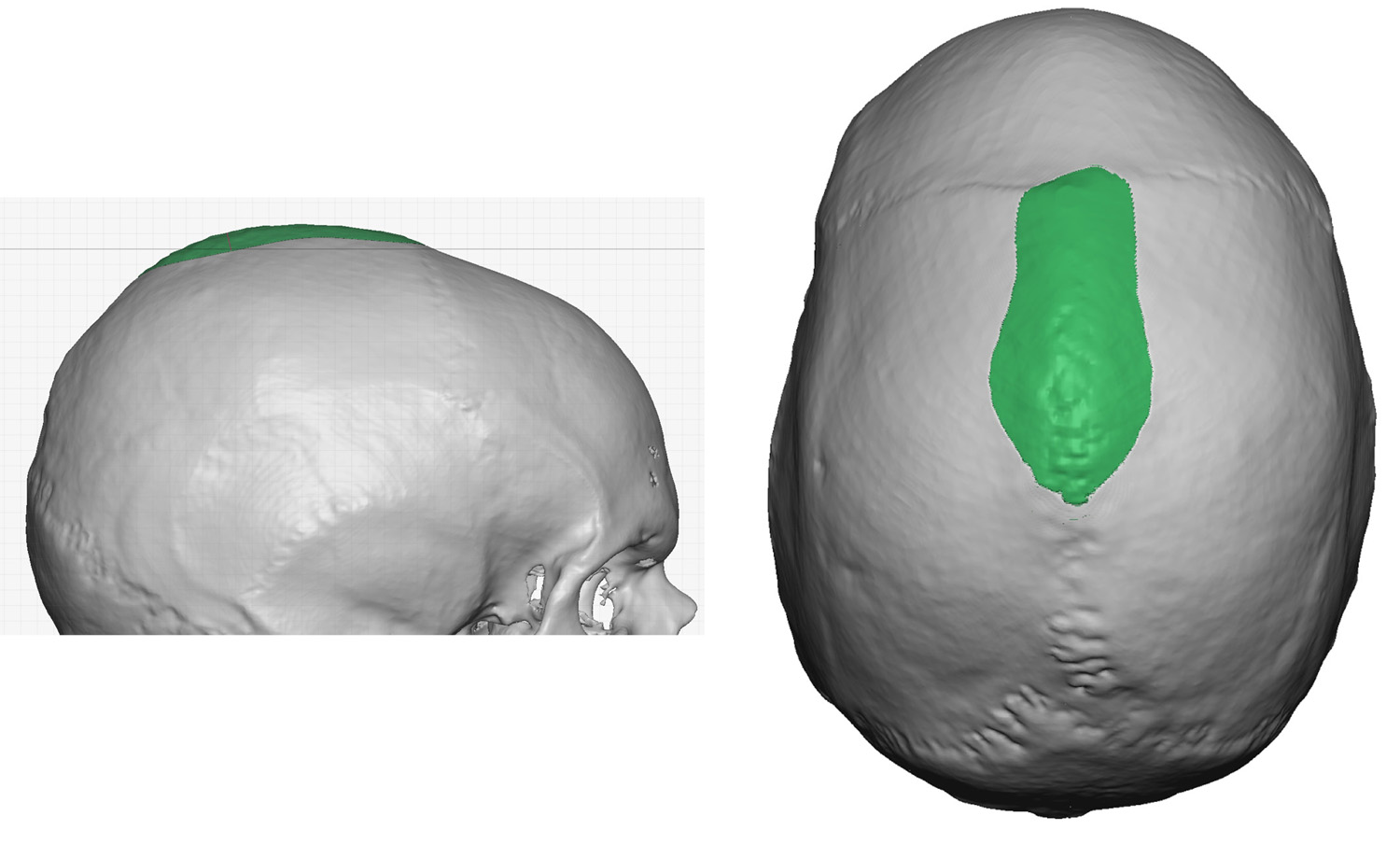
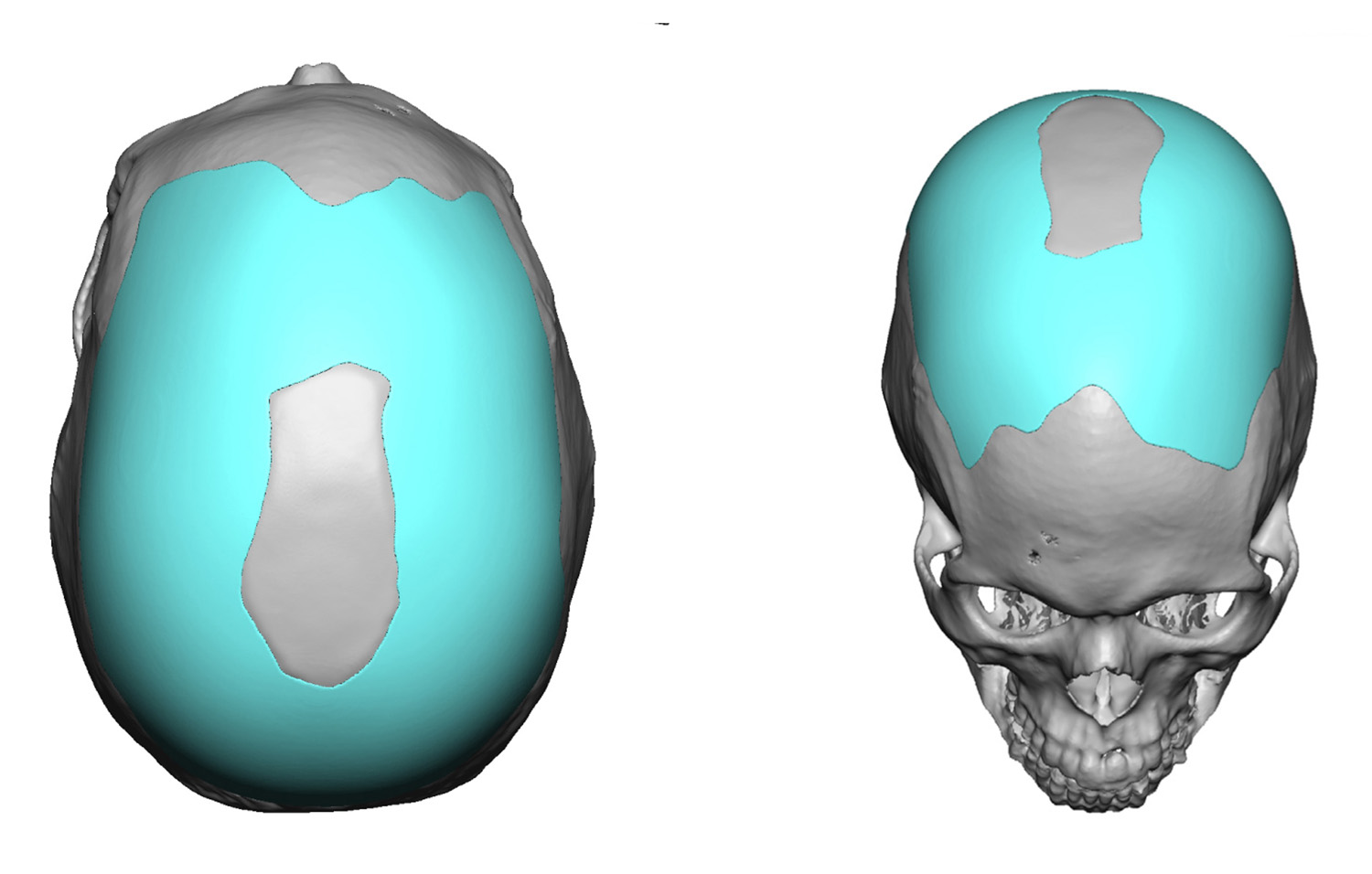 A two technique approach was proposed for his skull reshaping procedure including reduction of the sagittal crest and a custom skull implant placed around it. The custom skull implant built up both parasagittal regions as well as the upper occipital region and the very top of the forehead.
A two technique approach was proposed for his skull reshaping procedure including reduction of the sagittal crest and a custom skull implant placed around it. The custom skull implant built up both parasagittal regions as well as the upper occipital region and the very top of the forehead.
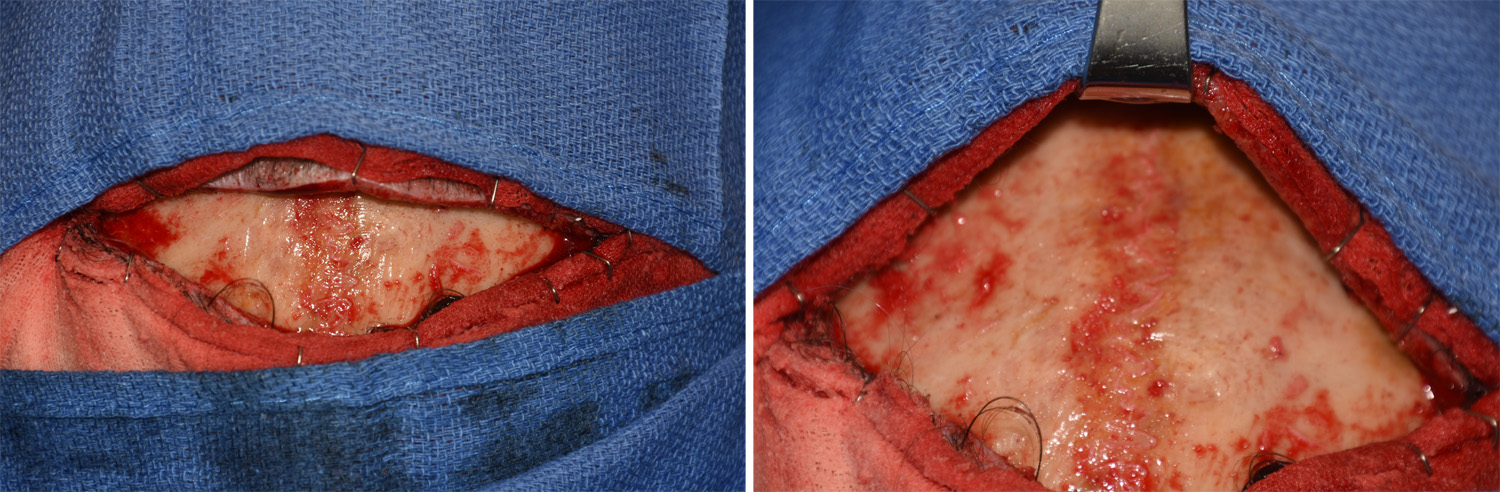
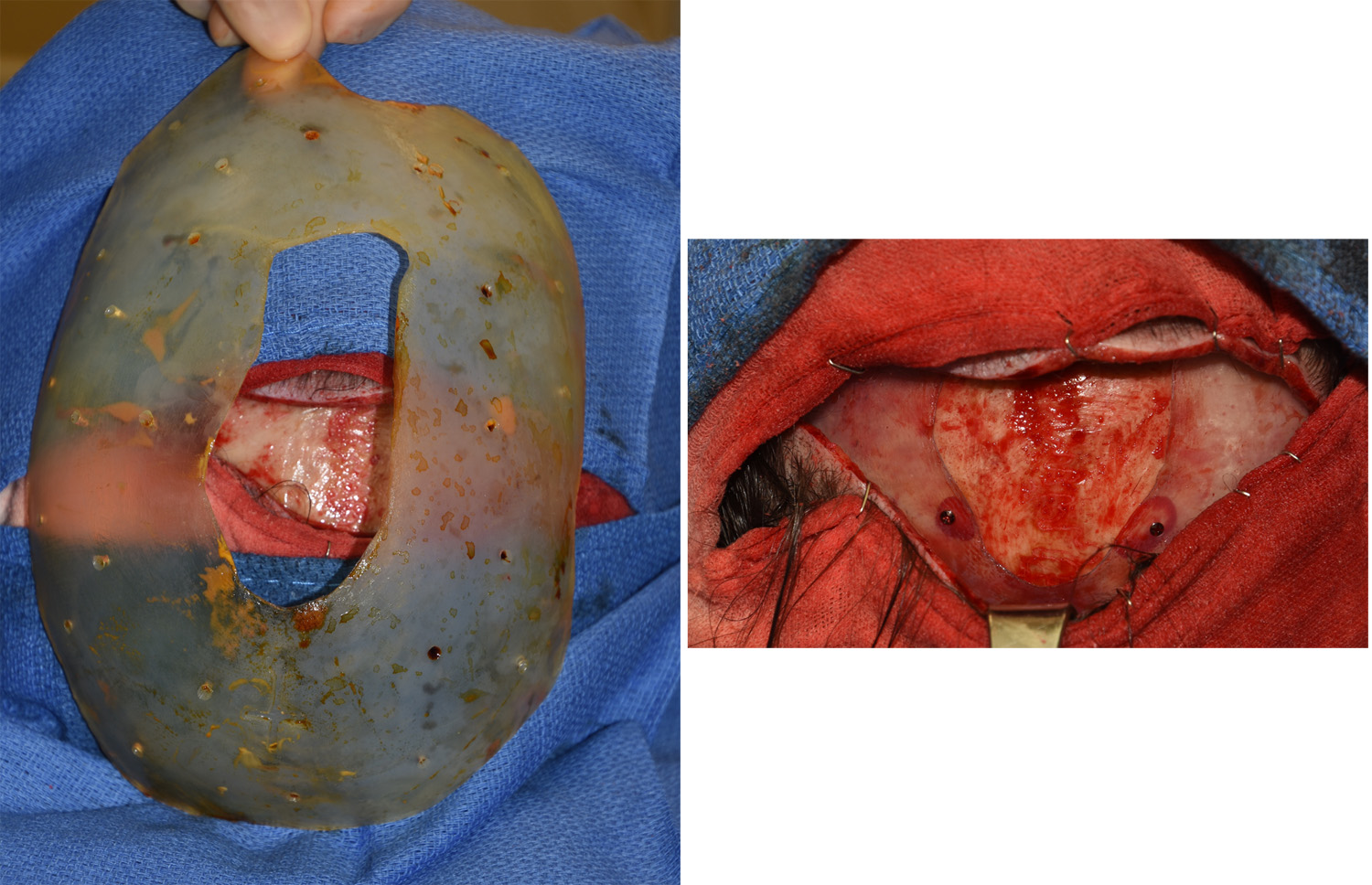 Under general anesthesia an 11 cm long scalp incision was made perpendicular to the sagittal crest across its highest point. Through this incision the height of the sagittal crest was reduced by 5 to 6mms down close to the diploic space. The fibrous suture line could be seen down into the bone. Once the sagittal crest was reduced, the custom skull implant was prepared by making multiple perfusion holes through it. It was then inserted and positioned around the reduced sagittal crest. It was secured into position by several 1.5 x 5mm microscrews.
Under general anesthesia an 11 cm long scalp incision was made perpendicular to the sagittal crest across its highest point. Through this incision the height of the sagittal crest was reduced by 5 to 6mms down close to the diploic space. The fibrous suture line could be seen down into the bone. Once the sagittal crest was reduced, the custom skull implant was prepared by making multiple perfusion holes through it. It was then inserted and positioned around the reduced sagittal crest. It was secured into position by several 1.5 x 5mm microscrews.
Custom skull implants can help create a more harmonious skull shape to build up low skull spots when combined with reduction of high bony areas. Many sagittal crest skull deformities must use this combined approach for the best result.
Highlights:
1) The sagittal crest skull deformity is marked by a high midline crest of bone surrounded by adjoining areas of skull deficiencies.
2) Sagittal crest skull reduction may not be enough to create a more convex head shape in the frontal view.
3) A custom parasagittal skull implant can be a complement to creating a better overall head shape in the sagittal crest skull reduction patient.
Dr. Barry Eppley
Indianapolis, Indiana