

Background: Chin augmentation with a sliding genioplasty is a well known aesthetic technique. It is not done as commonly as a chin implant but in the right patient has its own advantages. One of its benefits is that it brings the chin forward with its attached tongue-side musculature as well as lengthening the jawline. By so doing it can help smooth out the neck better than an implant which just pushes out the soft tissue chin pad and has no direct effect on the neck muscles behind it
The main muscles that a sliding genioplasty pulls forward is the genioglossus and geniohyoid. The genioglossus is a fan-shaped tongue muscle which comprises most of the tongue. Its origin is the spine on the back side of the chin bone and inserts into the hyoid bone and the bottom of the tongue. Its contraction enables one to stick their tongue out as well as enlarges the upper airway behind the base of the tongue. The geniohyoid muscle lies below the genioglossus but above the mylohyoid muscle. It runs from the back of the chin down to the hyoid bone and its contraction dilates the upper airway as it pulls the hyoid bone upward and forward.
Because of the attached muscles that accompany a sliding genioplasty, it could have an effect very similar to a direct muscle procedure used to treat obstructive sleep apnea. A genioglossus muscle advancement is an intrachin procedure where the genioglossus muscle is brought forward by using a window of bone in the chin. It is usually part of other obstructive sleep apnea procedures and is rarely done alone since obstructive sleep apnea almost always involves various structures at different areas of the airway. It is limited to a forward muscle movement that is no further than the thickness of the chin bone.
Case Study: This 46 year-old male presented with symptoms of obstructive sleep apnea and a short lower jaw. He wore CPAP at night. He had a class II malocclusion and an overall heavy face appearance. He was overweight but certainly not obese. He had significant daytime sleepiness. A sleep study showed multiple apneic episodes greater than 10 seconds and a drop in oxygen saturations to 84%. His apnea-hypopnea index (AHI) was 25. He did not want a maxillomandibular advancement.
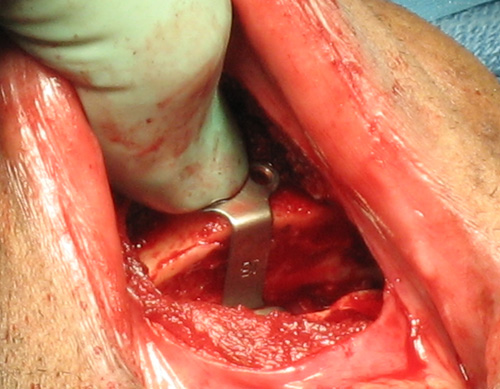 Under general anesthesia, an intraoral approach was used to deglove the chin. A mid-level near horizontal osteotomy bone cut was made through the chin keeping the muscles attached to the lingual side of the chin. The chin was brought forward 16mms and stabilized with central step plate as well as two side plates due to the magnitude of the movement.
Under general anesthesia, an intraoral approach was used to deglove the chin. A mid-level near horizontal osteotomy bone cut was made through the chin keeping the muscles attached to the lingual side of the chin. The chin was brought forward 16mms and stabilized with central step plate as well as two side plates due to the magnitude of the movement.
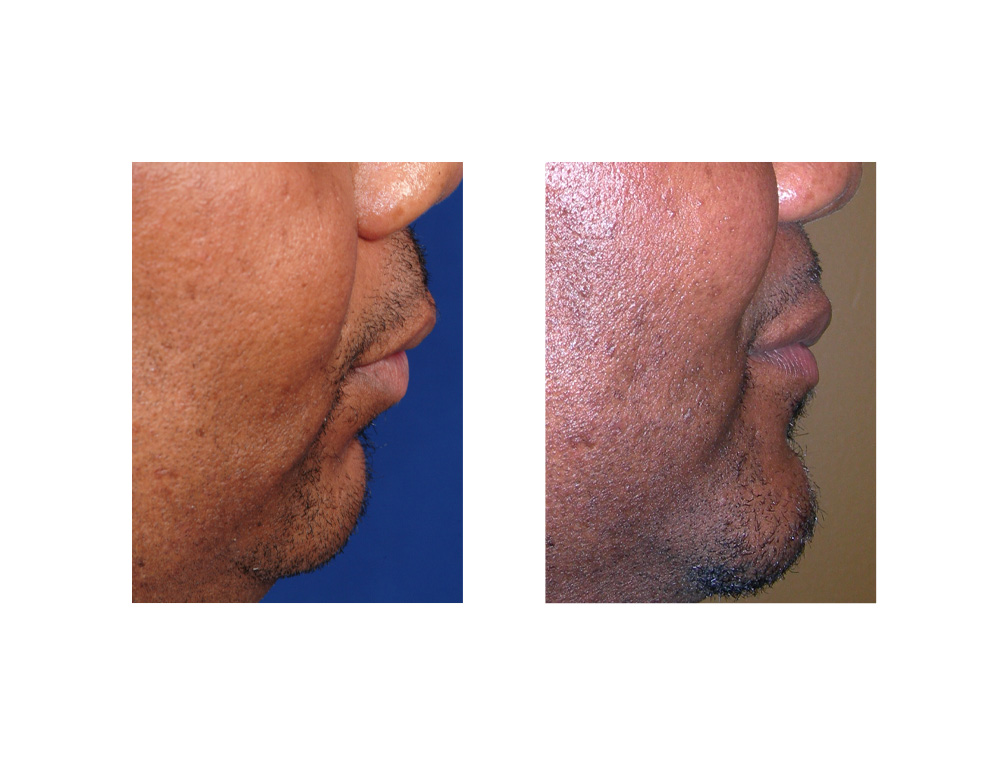 After surgery he had a significant increase in chin horizontal position and an improved facial profile. Despite the very large chin movement, his chin projection was not excessive. He had improvement in his sleep apnea symptoms but not a complete cure of it as was expected before surgery. His sleep study numbers improved to an AHI of 15.
After surgery he had a significant increase in chin horizontal position and an improved facial profile. Despite the very large chin movement, his chin projection was not excessive. He had improvement in his sleep apnea symptoms but not a complete cure of it as was expected before surgery. His sleep study numbers improved to an AHI of 15.
 For a genioglossus movement to be effective, its forward movement must be considerable. (greater than 15mms) This is not usually possible with the traditional technique of moving the genial tubercle alone. This sliding genioplasty was beneficial for this patient’s sleep apnea symptoms because of the magnitude of its movement. His initial lower jaw retrusion permitted a large sliding genoplasty movement.
For a genioglossus movement to be effective, its forward movement must be considerable. (greater than 15mms) This is not usually possible with the traditional technique of moving the genial tubercle alone. This sliding genioplasty was beneficial for this patient’s sleep apnea symptoms because of the magnitude of its movement. His initial lower jaw retrusion permitted a large sliding genoplasty movement.
Case Highlights:
1) A short chin and lower jaw is a known cause of obstructive sleep apnea.
2) The sliding genioplasty pulls the genioglossus muscle forward which can have a small secondary effect of bringing the base of the tongue forward as well to open the airway a bit.
3) For a sliding genioplasty to be helpful for sleep apnea the forward movement must be at least 10mms or greater.
Dr. Barry Eppley
Indianapolis, Indiana