

Defects of the outer skull produces indentations and depressions in the scalp or forehead. Skull deformities can be caused by a variety of sources including craniotomy surgery, fractures, and muscle atrophy (if in the temporal region) While hair can cover many of these issues, some patients will seek reconstruction of these cosmetic defects.
Building back out the skull bone, also known as cranioplasty, has been done for over a hundred years. Many materials have been used to onlay onto or over the defect including natural and synthetic bone, ceramics, calcium phosphate cements, and metallic plates and meshes. Which one is best is really a function of the surgeon’s expertise and experience and not so much what type of material is used as they all can be made to work.
 In most small to moderately-large cranial defects that are either partial or full-thickness, I prefer hydroxyapatite cements (HAC) or PMMA (poly methylmethacrylate) Both are liquid and powder mixtures that are turned into a slurry which can be molded to all margins. HAC is a bit trickier to work with but in a young patient may be better in the long-run as it is does allow for some tissue ingrowth through its fissures and cracks. PMMA is easier to work with and is quite fracture-resistant. It is also much less expensive which can be a significant advantage if one is paying out of pocket. In either case, I always put some powdered antibiotics into the mixtures for a slow release after surgery.
In most small to moderately-large cranial defects that are either partial or full-thickness, I prefer hydroxyapatite cements (HAC) or PMMA (poly methylmethacrylate) Both are liquid and powder mixtures that are turned into a slurry which can be molded to all margins. HAC is a bit trickier to work with but in a young patient may be better in the long-run as it is does allow for some tissue ingrowth through its fissures and cracks. PMMA is easier to work with and is quite fracture-resistant. It is also much less expensive which can be a significant advantage if one is paying out of pocket. In either case, I always put some powdered antibiotics into the mixtures for a slow release after surgery.
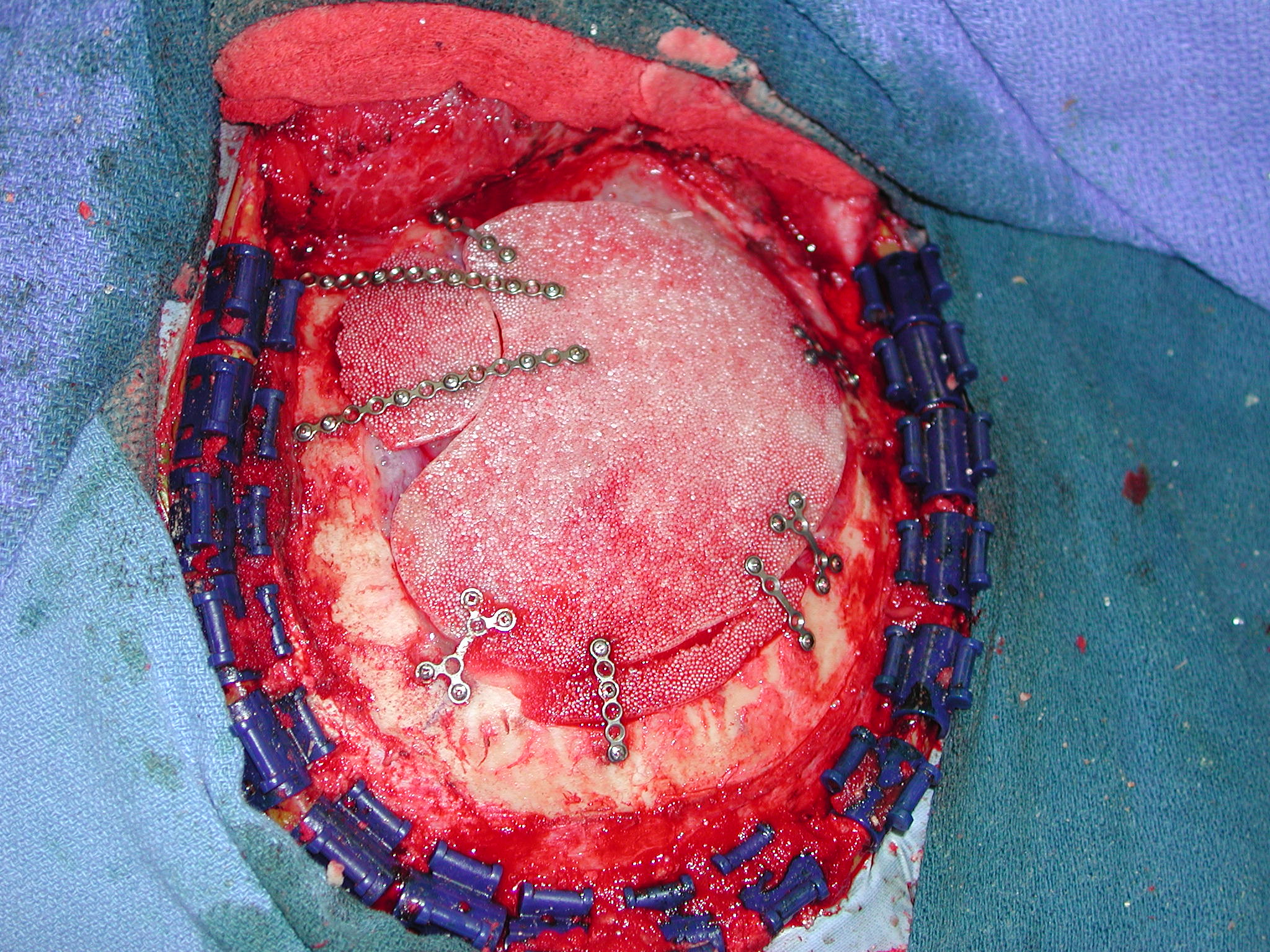
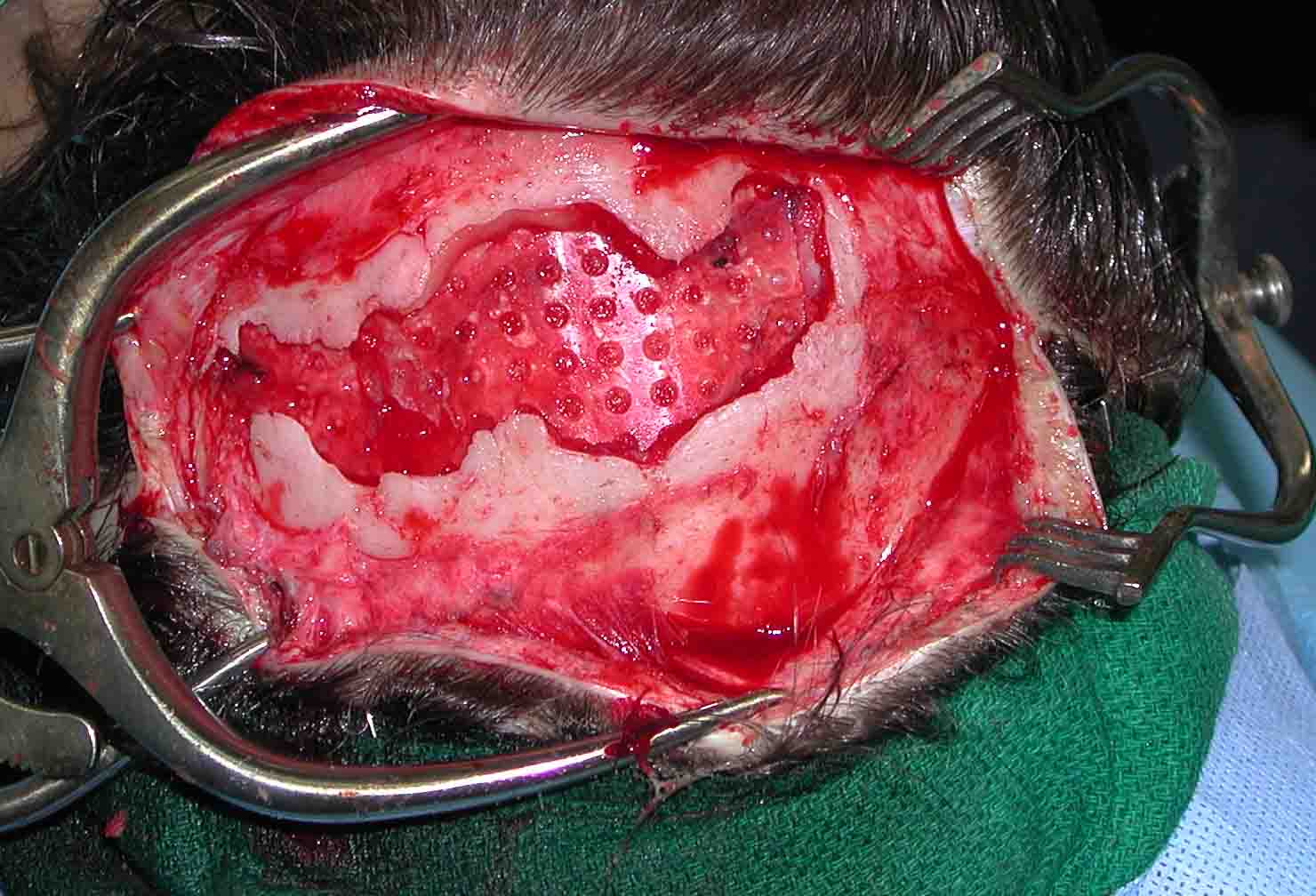
 In large full-thickness cranial defects, I have used computer-generated implants made of a porous material known as HTR. (hard tissue replacement) These are usually used in cases of loss of a craniotomy flap or for the immediate replacement of a skull bone tumor. The exactness of the computer imaging and modeling is quite impressive although most cases still require some minor modifications during surgery. The great benefit of HTR implants is that they allow for a lot of fibrovascular ingrowth which makes them resistant and/or treatable to infections should they develop. Bone ingrowth, while theoretically appealing, is usually of no practical significance due to the high fracture resistance of the material. When facing complex cranial defects, particularly of the forehead, cranial HTR implants have a long track history of clinical success.
In large full-thickness cranial defects, I have used computer-generated implants made of a porous material known as HTR. (hard tissue replacement) These are usually used in cases of loss of a craniotomy flap or for the immediate replacement of a skull bone tumor. The exactness of the computer imaging and modeling is quite impressive although most cases still require some minor modifications during surgery. The great benefit of HTR implants is that they allow for a lot of fibrovascular ingrowth which makes them resistant and/or treatable to infections should they develop. Bone ingrowth, while theoretically appealing, is usually of no practical significance due to the high fracture resistance of the material. When facing complex cranial defects, particularly of the forehead, cranial HTR implants have a long track history of clinical success.
Reconstruction of cranial defects is a highly successful procedure that can be done with a variety of materials. Synthetic bone substitute materials such as HAC and HTR produce very consistent results in experienced hands. These materials should be used with caution if there is predicted difficulty with scalp closure, if the patient has been irradiated or has a past history of osteoradionecrosis, or there has been an active or recent history of bone infection.
Dr. Barry Eppley
Indianapolis, Indiana