

Background: The hips are an important part of a female’s body and their shape is often very gender specific…women’s are curved while men are straight. To be specific, the hips refer to the anatomic region overlying the hip or femur-pelvic joint. It is located to the sides of the buttocks but below the iliac crest of the pelvic bone. Since the greater trochanter of the femur is the most lateral part of the bony hip region, the shape of the hips can be seen to be influenced by its prominence but not exclusively so. The natural amount of fat in the subcutaneous layer also helps determine the outer hip contour.
The aesthetic shape of the hips is almost an exclusively female concern. While too wide of hips is a more common aesthetic problem, there are females whose hips are too narrow or feel like they have ‘boy hips’. Hip augmentation is a way for those women to potentially enhance and widen their hips to create a more of an outer convex contour. Options for hip augmentation include fat grafting or hip implants.
Fat grafting through injection is the most common method today and is often part of many buttock augmentations as well. Through a liposuction harvest fat is collected and processed for injection. Through blunt cannulas the fat is injected to build out the hip contours. A side benefit is the body contouring that comes from the liposuction harvest. The downsides to the procedure are in how well does the fat survive after transfer and how much fat does one have to harvest. But if one has enough fat this is the best hip augmentation procedure despite the unpredictability of volume retention.
Since the fat comes from the patient’s own body, fat transfer is not ideal for patients with very little body fat. In these cases only silicone hip implants can be used. While their volume retention is assured, they come with all of the potential downsides that any other body implant has.
Case Study: This 36 year-old female wanted to fill out her hip depressions (trochanteric indentations) and get rid of her flanks. (love handles) She also had abdominal and waistline areas she wanted reduced although they were not an extensive amount of fat.
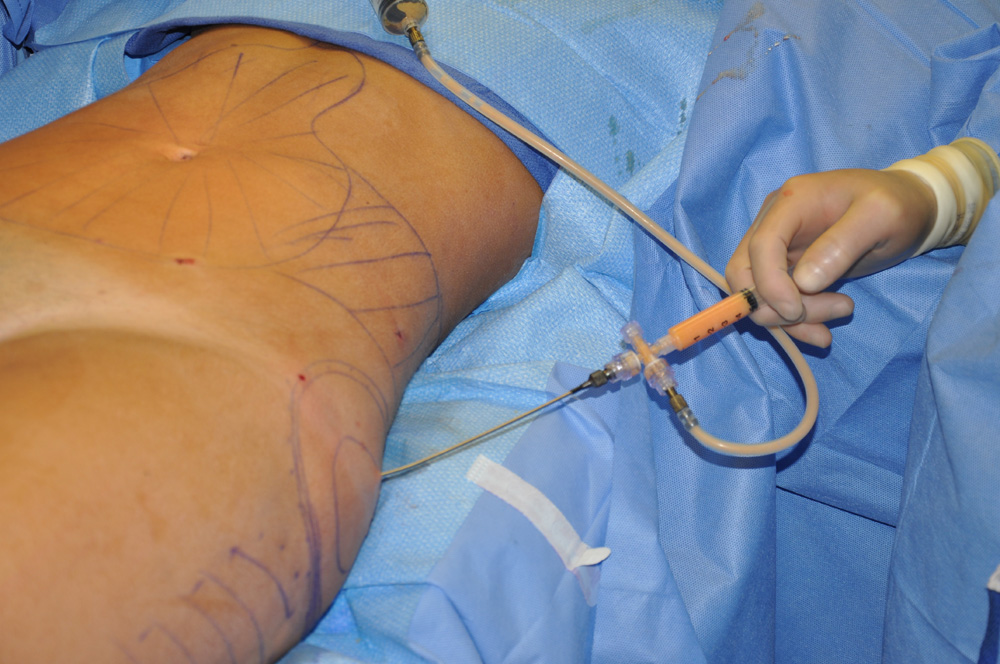 Under general anesthesia, liposuction was performed on her full abdomen, flanks and outer thighs. A total of 875cc of liposuction aspirate was obtained. This was processed down to 270cc of concentrated fat. Each hip indentation was injected with 135cc of fat through three separate angles in a linear fashion.
Under general anesthesia, liposuction was performed on her full abdomen, flanks and outer thighs. A total of 875cc of liposuction aspirate was obtained. This was processed down to 270cc of concentrated fat. Each hip indentation was injected with 135cc of fat through three separate angles in a linear fashion.
 While she did lose some of the initial fat injected, she remained with an improved hip contour at six months after the procedure. The very obvious indentations were gone and the outer hip contour had been changed into more of a convexity than a concavity. The combination of flank liposuction and hip augmentation made for a more pleasing shape.
While she did lose some of the initial fat injected, she remained with an improved hip contour at six months after the procedure. The very obvious indentations were gone and the outer hip contour had been changed into more of a convexity than a concavity. The combination of flank liposuction and hip augmentation made for a more pleasing shape.
Case Highlights:
1) Hip augmentation is most commonly performed for trochanteric depressions over the mid-hip area or to create a more rounded contour of flat hips.
2) Fat injections are the natural method of hip augmentation and require some fat to harvest.
3) Fat injections in the hips can be expected to retain 50% to 75% of the injected volume.
Dr. Barry Eppley
Indianapolis, Indiana