

The midface is a general term that is often used to refer to any structure between the eyes and the lower jaw, excluding that of the nose specifically. (even though it lies in the midface region) Anatomically it includes the infraorbital rims of the eyes, the zygoma and zygomatic arch and the maxilla down to the level of the teeth. These bone structures serve as the foundation for all of the overlying soft issues and have a major influence on their external appearance.
The common perception of aesthetic augmentation of the midface is that of cheek implants. Less commonly, tear trough and paranasal/pyriform aperture implants are known and used. While all of these standard midface implants have a role in aesthetic enhancements, they augment spot or selective areas of the midface on their respective bones. But they do not create a true midface augmentation effect and can’t because much of the midface skeletal structures are ‘left out’.
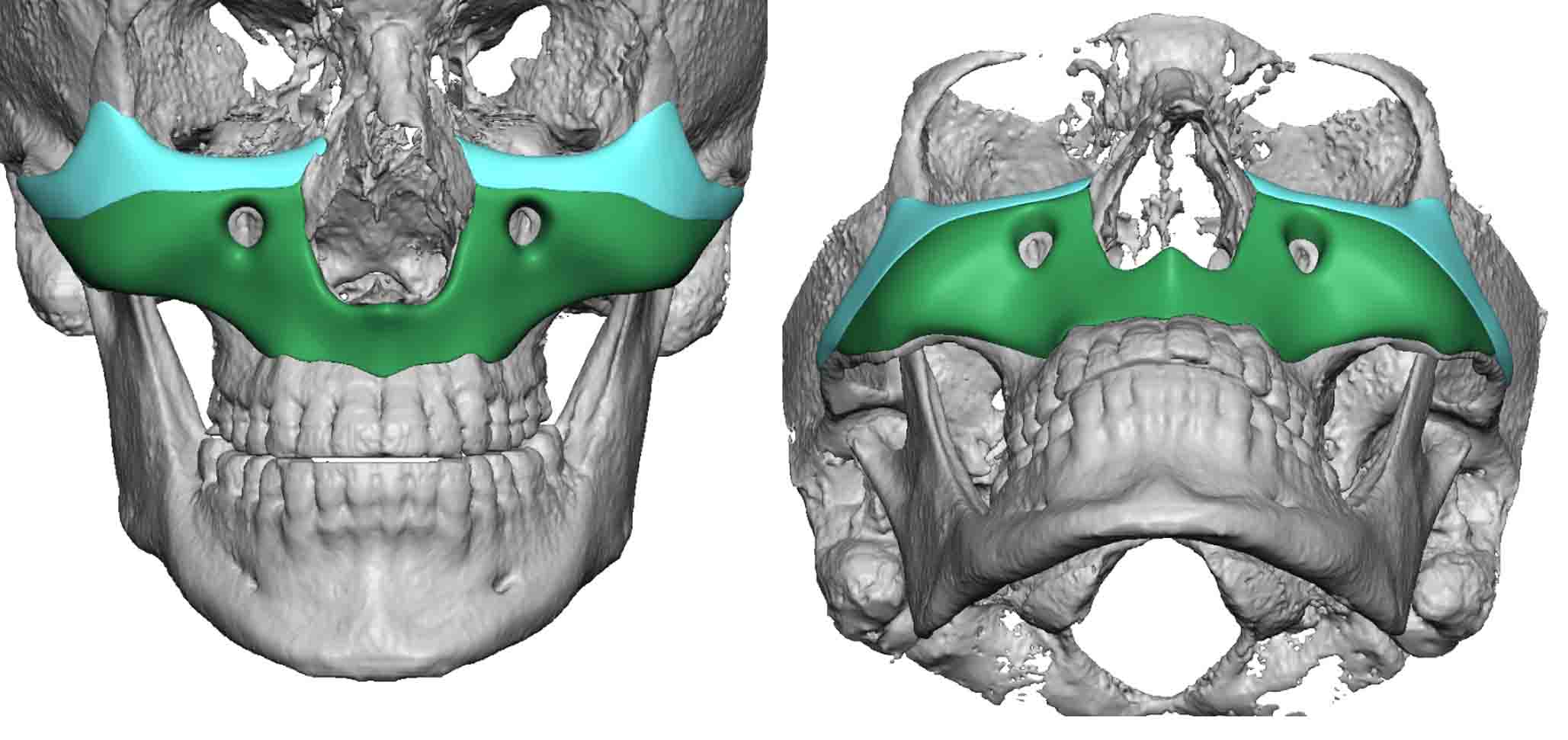
 Custom midface implants can be designed to be encompassing and can even be used to cover the entire midfacial skeleton. By so doing a true midface advancement can be achieved that is superior to a LeFort I osteotomy (minus the teeth and upper lip forward movements) or any combination of standard midface implants. Its changes are commensurate with a Left III osteotomy…again minus the teeth and an upper lip changes as well as the root of the nose.
Custom midface implants can be designed to be encompassing and can even be used to cover the entire midfacial skeleton. By so doing a true midface advancement can be achieved that is superior to a LeFort I osteotomy (minus the teeth and upper lip forward movements) or any combination of standard midface implants. Its changes are commensurate with a Left III osteotomy…again minus the teeth and an upper lip changes as well as the root of the nose.
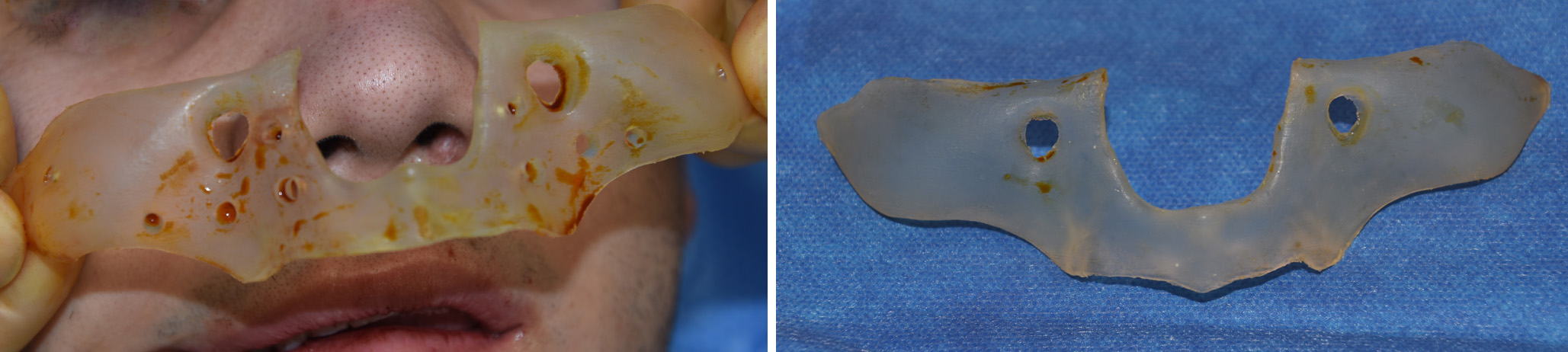
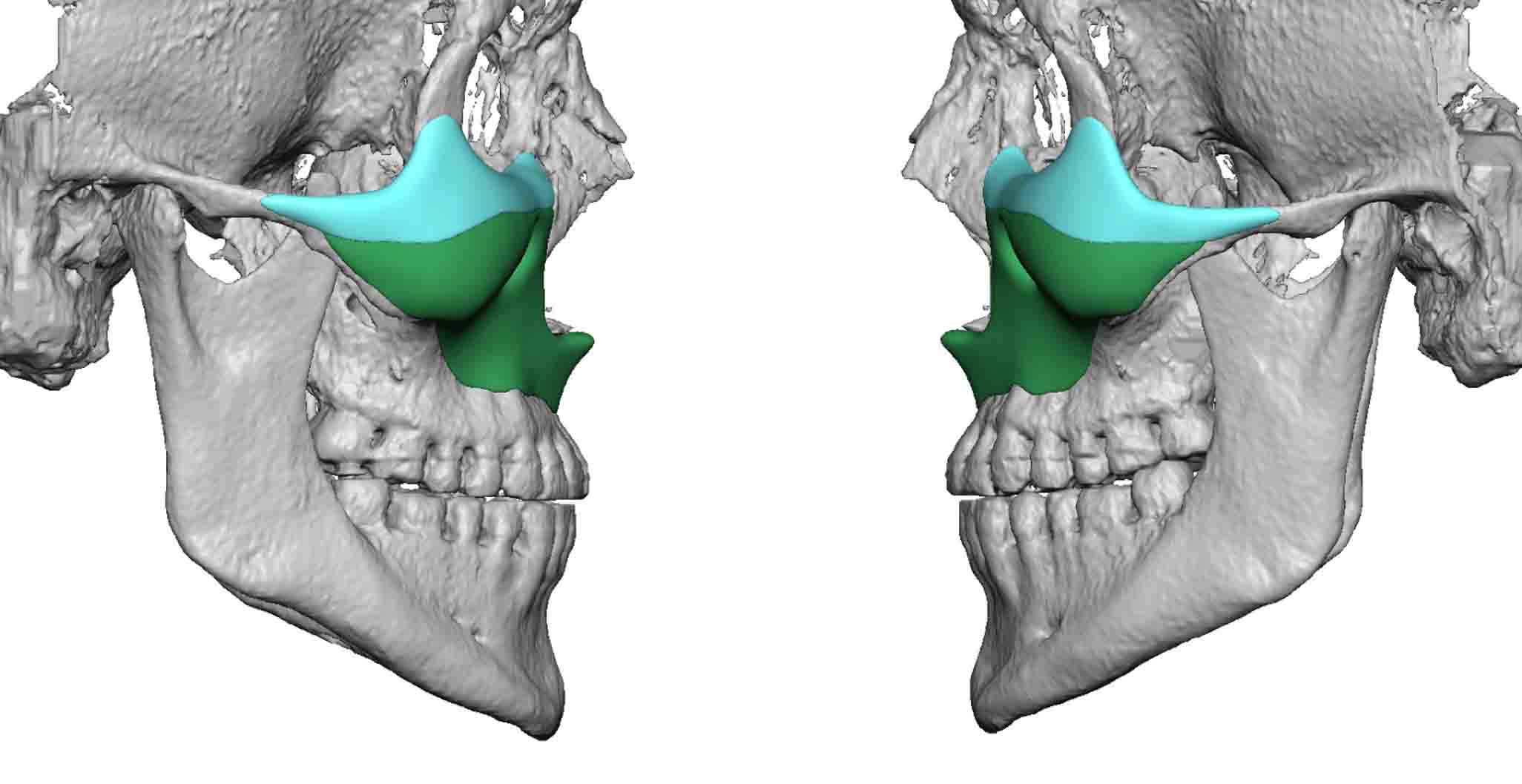
 A custom midface implant design must be so done thinking of how it will be inserted. In a complete midface implant (infraorbital-zygomatic-maxillary) it needs to be designed as two pieces and then assembled in the face. The lower part can be inserted through an intraoral approach.
A custom midface implant design must be so done thinking of how it will be inserted. In a complete midface implant (infraorbital-zygomatic-maxillary) it needs to be designed as two pieces and then assembled in the face. The lower part can be inserted through an intraoral approach.
 The top half of the implant, that encompasses the infraorbital and lateral orbital rims, is inserted through lower eyelid incisions. This is critical point of access because the implant must be properly positioned on top of the infraorbital rims. (which is very hard to do from below)
The top half of the implant, that encompasses the infraorbital and lateral orbital rims, is inserted through lower eyelid incisions. This is critical point of access because the implant must be properly positioned on top of the infraorbital rims. (which is very hard to do from below)
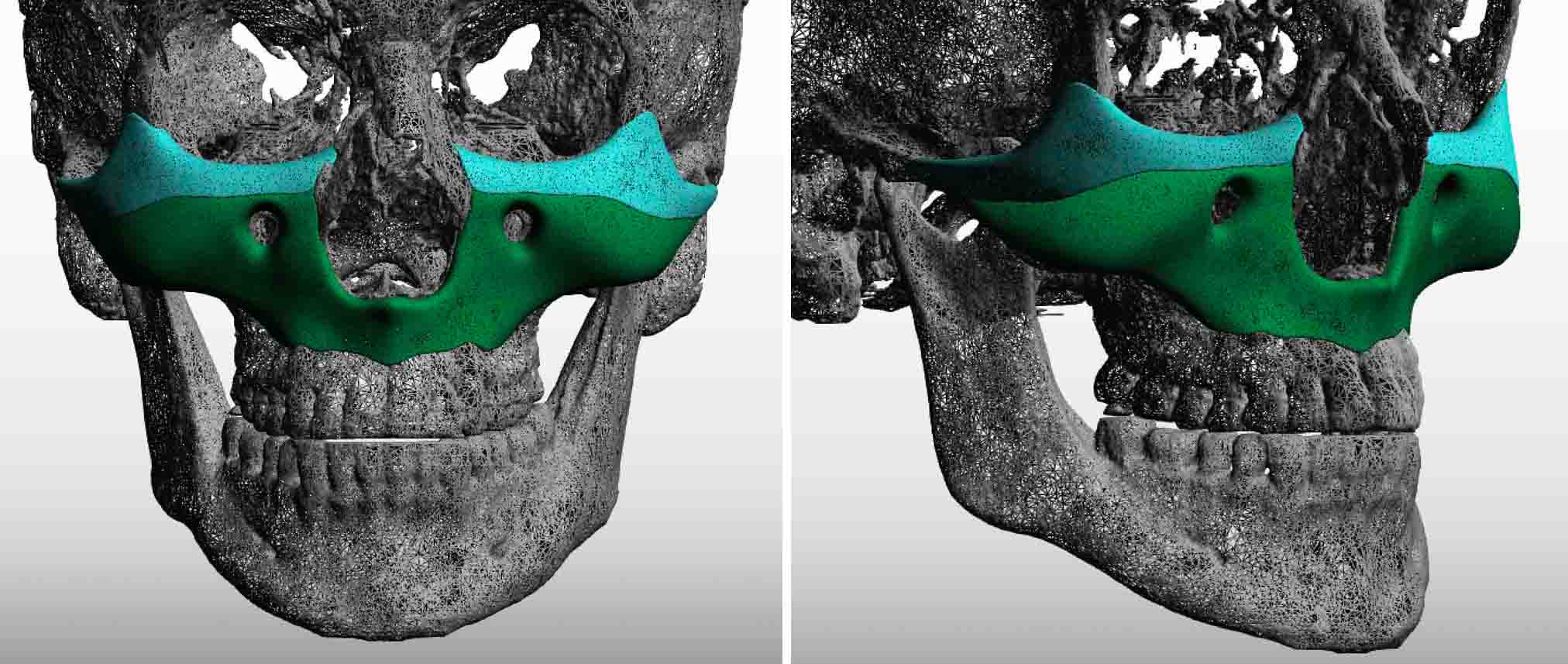
They are many variations of how a complete custom midface implant can be designed. But the approach of making it a two piece design offers the opportunity for complete bony coverage with the assurance of proper placement of the implant with good fixation.
Dr. Barry Eppley
Indianapolis, Indiana