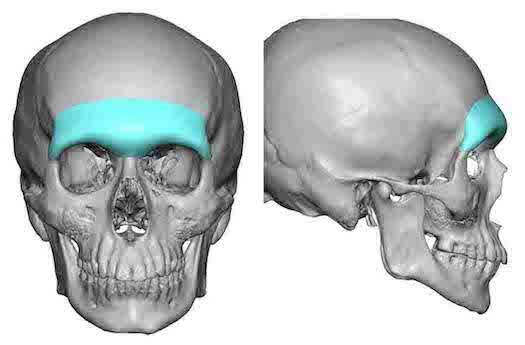


One distinct male feature is the of a prominent brow bone at the lower end of the forehead. It is one of many facial features that distinguishes males from females. It extends over the eyes with a horizontal projection, has a brow bone break before heading up into the forehead and has a slight glabellar depression between the medial brow bone prominences.
In today’s male beauty trends many models display a very strong or exaggerated brow bone appearance. It borders on being an almost angry appearance but is better anatomically described as an ultra low brow bone projection with near complete coverage of the upper eyelids. While I frequently get requests for such a brow bone augmentative change, I have to advise that such requests are almost always impossible to achieve. This is due to the fact the soft tissues of the eyebrows are tight and can not be driven down below the existing brow bones unless these tissues have been first expanded before a brow bone implant is placed.
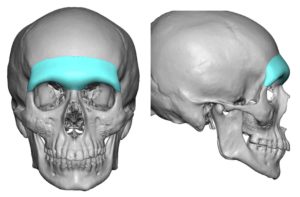
More realistic brow bone augmentation results create less dramatic changes but appreciable improvements nonetheless. More horizontally oriented projection across the orbital rims, a brow bone break and a more distinct corner or tail of the brow bone are achievable augmentative changes.
 While brow bone implants have been done using different materials, there is no questions today that a custom brow bone implant technique is the far superior method. Besides creating an assured smooth preformed shape, the implant can be placed through the smallest incisions possible….a critical need in the male patient.
While brow bone implants have been done using different materials, there is no questions today that a custom brow bone implant technique is the far superior method. Besides creating an assured smooth preformed shape, the implant can be placed through the smallest incisions possible….a critical need in the male patient.
Custom brow bone implants usually require a three incision placement technique, all of which are small and heal inconspicuously. The key is to get the implant low enough over the brow bones through adequate soft tissue release and good positioning and fixation over the lateral orbital rims. One may think this can be done exclusively from a superior approach only…but that can be ill-advised if the brow bone implant goes any length along the lateral orbital rims.
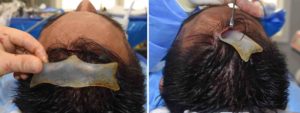
 My preferred approach is to make an initial 2 cm incision in the midline behind the frontal hairline. Endoscopic-assisted subperiosteal dissection is done over the entire forehead and across the brow bones. The periorbita is released from side to side and the supraorbital nerves identified and released from the bone. If the implant goes any distance along the lateral orbital rim, the dissection is completed by making small upper eyelid incisions in a lateral skin crease. This ensures that the tails of the implant are properly positioned down to the frontozygomatic suture and the entire implant is positioned low enough over the supraorbital rims. Small screw fixation is used to secure the implants on the lateral orbital rim. If only a superior incisional approach is used a percutaneous endoscopic-assisted screw placement is done in the glabellar region.
My preferred approach is to make an initial 2 cm incision in the midline behind the frontal hairline. Endoscopic-assisted subperiosteal dissection is done over the entire forehead and across the brow bones. The periorbita is released from side to side and the supraorbital nerves identified and released from the bone. If the implant goes any distance along the lateral orbital rim, the dissection is completed by making small upper eyelid incisions in a lateral skin crease. This ensures that the tails of the implant are properly positioned down to the frontozygomatic suture and the entire implant is positioned low enough over the supraorbital rims. Small screw fixation is used to secure the implants on the lateral orbital rim. If only a superior incisional approach is used a percutaneous endoscopic-assisted screw placement is done in the glabellar region.

 Satisfying aesthetic results from custom brow bone implants are consistently obtained as long as the patient recognizes that reliable augmentation can be obtained in horizontal projection with some limited inferior brow fullness.
Satisfying aesthetic results from custom brow bone implants are consistently obtained as long as the patient recognizes that reliable augmentation can be obtained in horizontal projection with some limited inferior brow fullness.
Dr. Barry Eppley
Indianapolis, Indiana