

Background: Orthognathic surgery is the collection of facial osteotomy procedures that have been done for more than fifty years. One of the most commonly performed is the sagittal split ramus osteotomy or the SSRO. This incredibly clever osteotomy design, as the name implies, sections the ramus or angle area of the lower jaw into two pieces sagittally. The separation of the proximal non-tooth bearing condylar-ramus bone segment from the distal tooth bearing ramus-body segment allows the lower jaw to be sagittally changed in length. The lower jaw length change, albeit longer or shorter, is determined by the establishment of a better occlusal relationship.
Once the occlusion is set in an SSRO, the ramus segments are stabilized with plate and screw fixation. In many cases this results in the recreation of smooth inferior border line from the most posterior jaw angle point all the way to the chin. But this does not always occur for a variety of reasons. The way the ramus segments were positioned intraoperatively, the type of dimensional movement that occurs when the distal bone segment is moved into occlusion and any volumetric bone loss from the soft tissue stripping needed to perform the procedure. Also, since an SSRO procedure produces a two-dimensional change in position it can not create any width changes or reliably improve the symmetry between the two jaw angle shapes.
As a result of all of these potential issues, it is not rare that jaw angle asymmetries and inferior border irregularities occur. These are not improvable by any additional bone procedures.

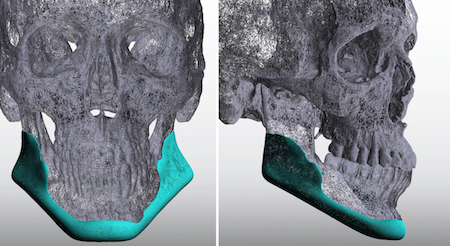
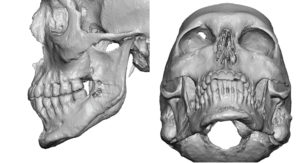 Case Study: This male had a prior history of orthognathic surgery consisting of a sagittal split ramus osteotomy and a bony genioplasty. While its occlusion was improved his lower jawline was asymmetric at the angles and chin. His jawline was also very narrow from the front view.
Case Study: This male had a prior history of orthognathic surgery consisting of a sagittal split ramus osteotomy and a bony genioplasty. While its occlusion was improved his lower jawline was asymmetric at the angles and chin. His jawline was also very narrow from the front view.
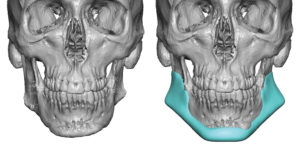
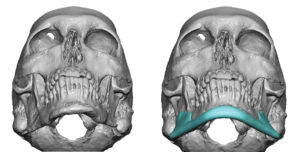 A 3D CT scan was used to create a custom jawline implant that corrected the chin and jaw angle asymmetry, improved jaw angle prominence as well as widened his jawline.
A 3D CT scan was used to create a custom jawline implant that corrected the chin and jaw angle asymmetry, improved jaw angle prominence as well as widened his jawline.
 The custom jawline implant was placed through a three incisional placement technique (submental skin and bilateral posterior vestbibular intraoral incisions) in a front to back direction.
The custom jawline implant was placed through a three incisional placement technique (submental skin and bilateral posterior vestbibular intraoral incisions) in a front to back direction.
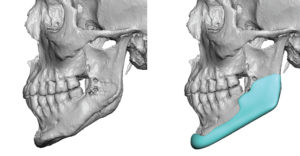
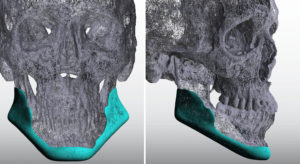 Smoothing out the jawline and correcting asymmetries can only be done by a custom jawline implant design. Such a wraparound implant is very much like building out the bone contour along the inferolateral border. Further enhancements can be done at the same time but the base concept of the design is for symmetry correction.
Smoothing out the jawline and correcting asymmetries can only be done by a custom jawline implant design. Such a wraparound implant is very much like building out the bone contour along the inferolateral border. Further enhancements can be done at the same time but the base concept of the design is for symmetry correction.
Case Highlights:
1) The sagittal split osteotomy is the most commonly performed lower jaw orthognathic surgery.
2) The sagittal splint osteotomy due to disruption of the ramus bone structure is prone to jaw angle shape deformities.
3) Creating a smoother and more symmetric jawline after orthognathic surgery can be done by the design and placement of a custom jawline implant.
Dr. Barry Eppley
Indianapolis, Indiana