

Body contouring in the waist region is currently restricted to modifications of skin and fat. The traditional procedures of liposuction and various forms of tummy tucks work well when excess fat and skin exists from weight loss, pregnancies and genetic body shapes have created the opportunities for those procedures to be used. But when little fat or loose skin exists or when traditional procedures have still not created the desired inward curvature a more structural approach is needed.
 Rib removal is the only structural reductive procedure for the waistline. It is a surgery that is associated with a lot of skepticism about its safety and effectiveness although there is actual little reported clinical experience with it. There has yet to be a definitive study of the relationship of the lower ribcage to the waistline and which ribs have the greatest impact on improving its shape. The free floating #11 and #12 ribs are always been touted as the ribs to treat but is this due to convenience or effectiveness?
Rib removal is the only structural reductive procedure for the waistline. It is a surgery that is associated with a lot of skepticism about its safety and effectiveness although there is actual little reported clinical experience with it. There has yet to be a definitive study of the relationship of the lower ribcage to the waistline and which ribs have the greatest impact on improving its shape. The free floating #11 and #12 ribs are always been touted as the ribs to treat but is this due to convenience or effectiveness?
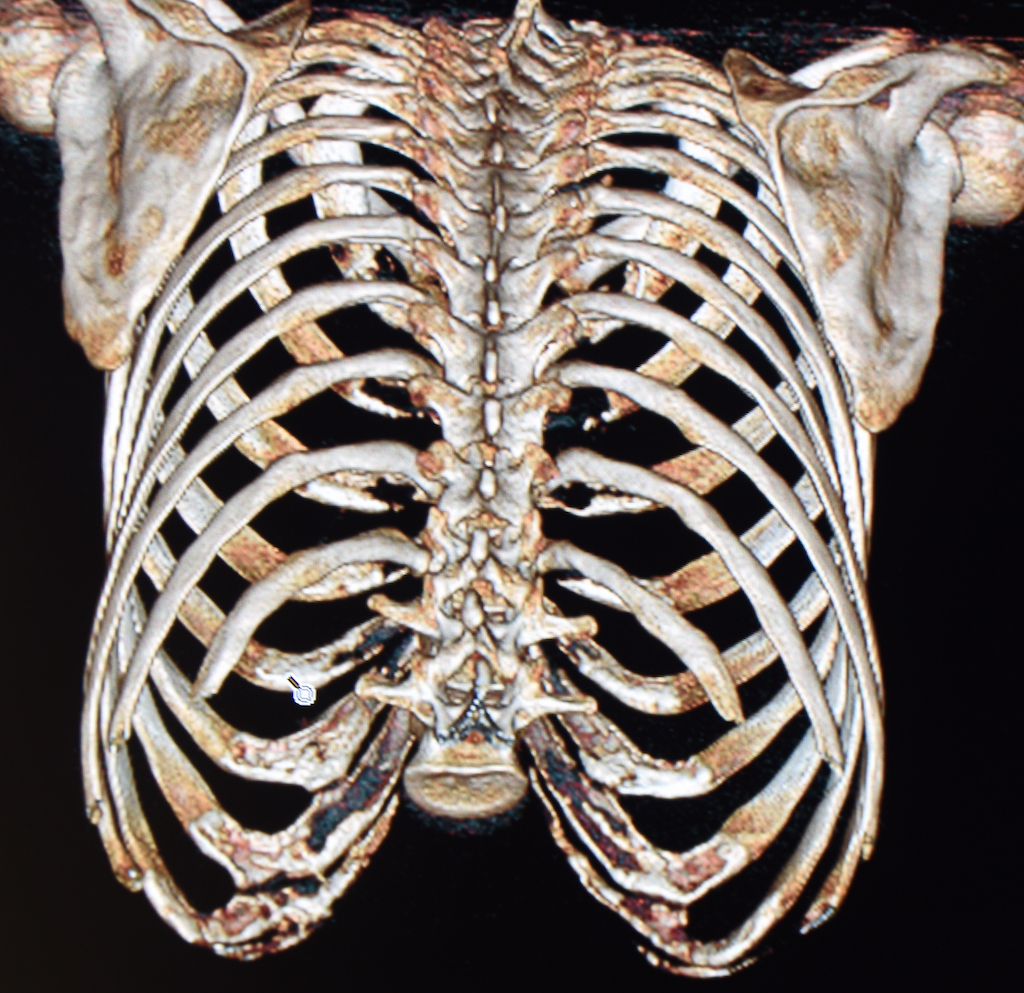
In the Global Open November 2023 issue of the journal Plastic and Reconstructive Surgery an article on this topic was published entitled ‘Anatomical Bases for Aesthetic Costal Surgery: Assessing the Thoracoabdominal Limits.’ In this paper the authors analyzed 83 female thoracoabdoiminal CT scans and made various measurements of the lower ribcage (ribs #10,11 and 12) that were closest to the waistline.
Their clinical findings were as follows:
- The lower ribs are the immovable pillars of the waist.
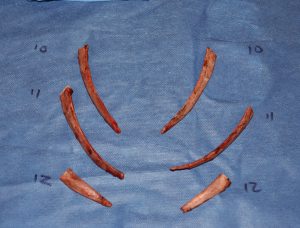
- Rib #10 is the longest of the lower ribs, has the most bone mass, may have the greatest impact on waist reduction, and has the potential for the highest risk of complications with removal.
- While ribs #11 and #12 are shorter than #10 their removal still has value in waist reduction.
- If the lengths of the ribs are removed the thickness measurement of the thoracoabdominal wall is reduced by approximately 30%.
- Dissection may be more difficult in ribs #10 and #11 due to the increased muscle insertions.
- Rib #12 was the pair of ribs that exhibited asymmetry with partial agenesis on one side.
- Rib removal embellishes the shape of the hips by reducing the thickness of the abdominal wall.
This is the first anatomic study that has evaluated the basis for rib modification surgery for waist reduction. By the author’s own admission this is a descriptive study but it is very interesting from my clinical experience having removed hundreds of ribs for such waist reduction. Merging this experience with this anatomic study I can say the following:
 Rib #12 is well known to be the shortest rib and, having seen two cases of rib #12 agenesis discovered intraoperatively, one needs to be aware of this possibility. Deep palpation may be able to reveal the shortness of rib #12 preoperatively but this is only useful in the thinnest of patients. While it would be ideal to have every patient undergo a 3D CT scan of the ribcage this does add to the cost of the surgery.
Rib #12 is well known to be the shortest rib and, having seen two cases of rib #12 agenesis discovered intraoperatively, one needs to be aware of this possibility. Deep palpation may be able to reveal the shortness of rib #12 preoperatively but this is only useful in the thinnest of patients. While it would be ideal to have every patient undergo a 3D CT scan of the ribcage this does add to the cost of the surgery.- There is no question that the longer of the lower ribs (#10 and #11) provides the best impact on decreasing the rigidity of the lateral abdominal wall by the sheer removal of bone mass and extensive loss of muscular attachments
- While rib #10 has great value in waist reduction due to its downward angulation the authors did not investigate the relationship of the pleura of the lung to this rib. This is the rib where pleural violation can occur because of its close relationship. I have seen the pleura several times at rib #10 but never at rib #11.
- When possible ribs #10, 11 and 12 should be taken with rib #12 being the least important but the easiest one to remove due to its shorter length.
- What the relationship is between loss of rib support and decrease in waist shape is not completely predictable. This study shows a potential 30% loss of thickness in the abdominal wall with rib removal. How much waist reduction can occur is undoubtably reflective of how thick the soft tissues are between the skin and the ribs. The thicker this softy tissue layer is the less impact rib removal will have.
- This study did not evaluate the impact of the latissimus dorsi muscle on waist shape. This very thick muscle extends beyond that of the ribs and makes a significant contribution to the outer contour of the waist. It is a soft tissue element that I always reduce with rib removal surgery because of this effect.
 Rib #12 is well known to be the shortest rib and, having seen two cases of rib #12 agenesis discovered intraoperatively, one needs to be aware of this possibility. Deep palpation may be able to reveal the shortness of rib #12 preoperatively but this is only useful in the thinnest of patients. While it would be ideal to have every patient undergo a 3D CT scan of the ribcage this does add to the cost of the surgery.
Rib #12 is well known to be the shortest rib and, having seen two cases of rib #12 agenesis discovered intraoperatively, one needs to be aware of this possibility. Deep palpation may be able to reveal the shortness of rib #12 preoperatively but this is only useful in the thinnest of patients. While it would be ideal to have every patient undergo a 3D CT scan of the ribcage this does add to the cost of the surgery.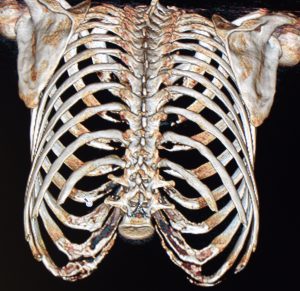
 When possible ribs #10, 11 and 12 should be taken with rib #12 being the least important but the easiest one to remove due to its shorter length.
When possible ribs #10, 11 and 12 should be taken with rib #12 being the least important but the easiest one to remove due to its shorter length.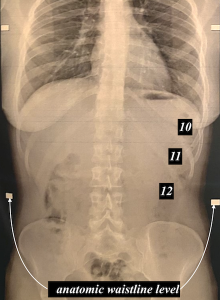 This study provides an anatomic basis for the benefits of structural reduction for waist reshaping in select patients when traditional body contouring methods are either not an option or have have proven ineffective. While it is logical to assume that ribs 11 and 12 are what is needed to achieve this effect, clinical experience has shown that rib #10 is equally important even though by x-ray it appears superior to the actual waistline. This is because of its severe angulation downward and that it actually sticks out further than the two ribs below it.
This study provides an anatomic basis for the benefits of structural reduction for waist reshaping in select patients when traditional body contouring methods are either not an option or have have proven ineffective. While it is logical to assume that ribs 11 and 12 are what is needed to achieve this effect, clinical experience has shown that rib #10 is equally important even though by x-ray it appears superior to the actual waistline. This is because of its severe angulation downward and that it actually sticks out further than the two ribs below it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon