

The most simplest definition of vertical orbital dystopia is that the eyes do not lie on the same horizontal plane. While it could be that the abnormal eye sits too high, it is far more common that the vertical direction of deformity is that it sits lower than the opposite normal eye. This can occur for a variety of reasons including developmental, traumatic or tumor resection reasons. But for ‘aesthetic’ vertical orbital dystopia it occurs as part of a developmental facial asymmetry (hypoplasia) and is in the range of a 2 to 6mm horizontal discrepancy.
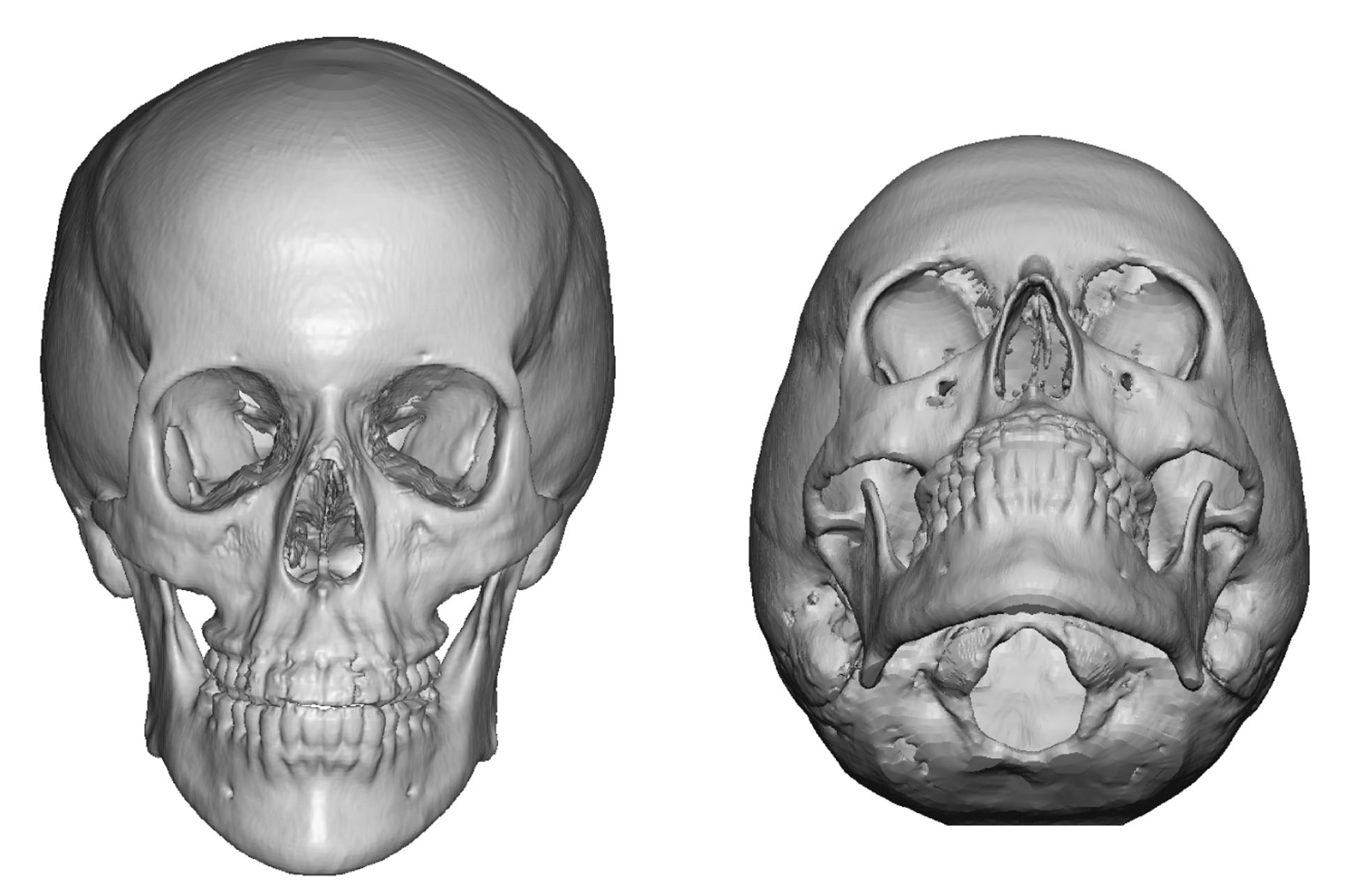 It is important to realize that it is the entire orbital box and its attached surrounding structures that are affected and not just the eyeball and the orbital floor in isolation. This is most easily appreciated in a 3D CT scan where the infraorbital rim, cheek and even the brow bone (top of the box) sits lower. With that also comes issues with the surrounding soft tissues with alterations in upper and lower eyelid positioning and a lower eyebrow as well.
It is important to realize that it is the entire orbital box and its attached surrounding structures that are affected and not just the eyeball and the orbital floor in isolation. This is most easily appreciated in a 3D CT scan where the infraorbital rim, cheek and even the brow bone (top of the box) sits lower. With that also comes issues with the surrounding soft tissues with alterations in upper and lower eyelid positioning and a lower eyebrow as well.

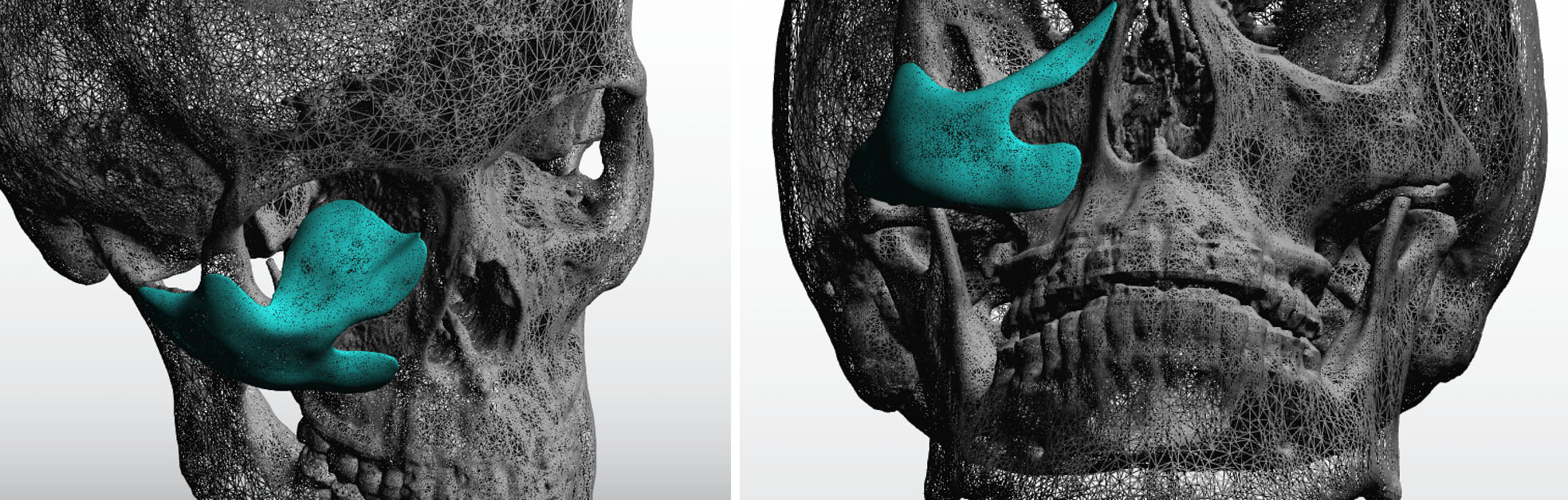 With such a 360 degree problem the treatment plan for vertical orbital dystopia surgery must factor in all components of the problem for the most successful improvement. From a skeletal standpoint the most complete correction involves the orbital floor, infraorbital rim and adjoining anterior cheek. This is best done with a custom implant made from the patient’s 3D CT scan. Whether one should optimize the correction with perfectly designed symmetry of the implant depends on how much eye elevation is needed and whether the position of the eyelids is to be addressed as well either concurrently or secondarily. (for example if the eyelid is being significantly this may create upper eyelid ptosis and/or increased scleral show of the lower eyelid)
With such a 360 degree problem the treatment plan for vertical orbital dystopia surgery must factor in all components of the problem for the most successful improvement. From a skeletal standpoint the most complete correction involves the orbital floor, infraorbital rim and adjoining anterior cheek. This is best done with a custom implant made from the patient’s 3D CT scan. Whether one should optimize the correction with perfectly designed symmetry of the implant depends on how much eye elevation is needed and whether the position of the eyelids is to be addressed as well either concurrently or secondarily. (for example if the eyelid is being significantly this may create upper eyelid ptosis and/or increased scleral show of the lower eyelid)
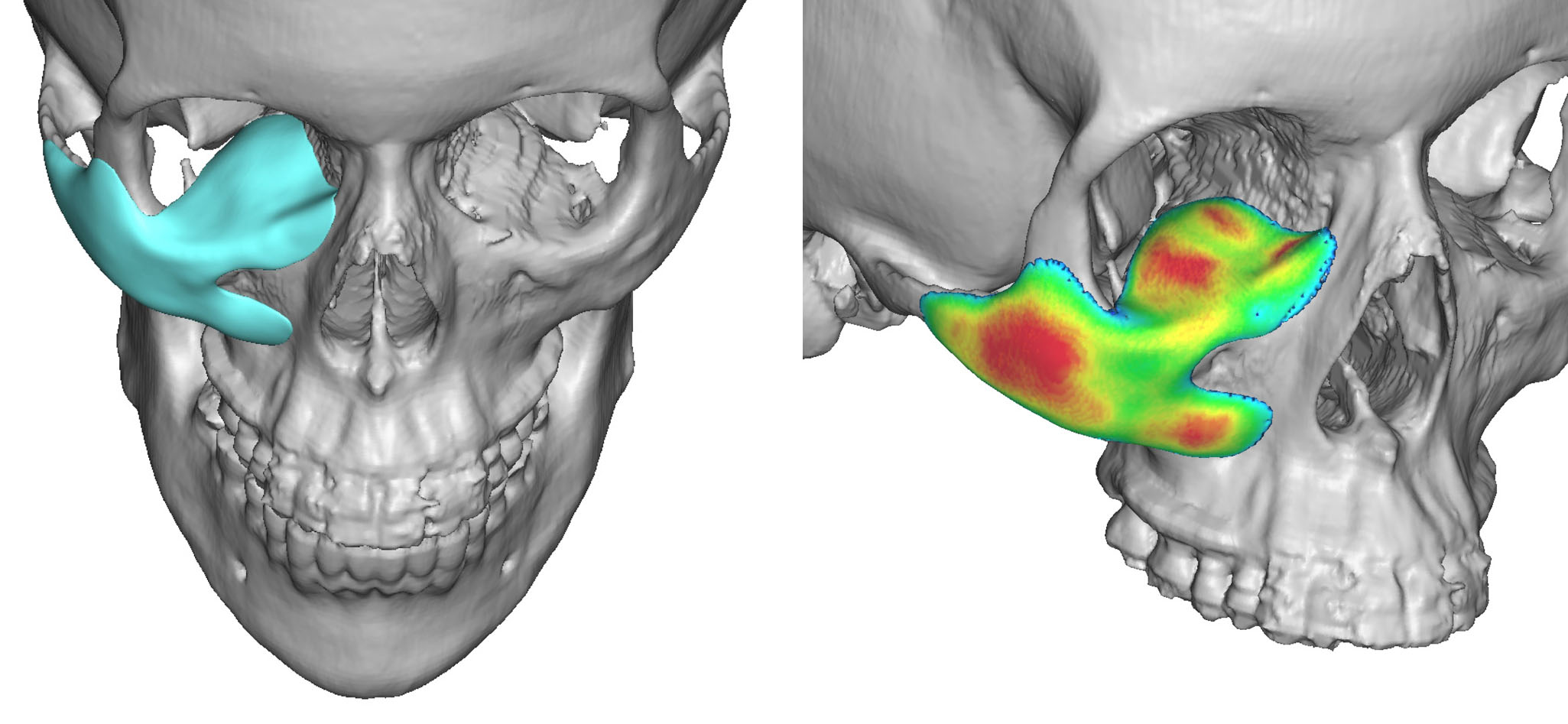 A custom 3D implant for vertical orbital dystopia is placed through a subciliary lower eyelid incision. It can be placed without disruption of the current lateral cantonal attachment although that may need to elevated as well if a concurrent lower eyelid repositioning is needed as well. I prefer to use small titanium microscrews or fixation of the implant along the infraorbital rim and cheek so that it lays completely flat along all bone surfaces.
A custom 3D implant for vertical orbital dystopia is placed through a subciliary lower eyelid incision. It can be placed without disruption of the current lateral cantonal attachment although that may need to elevated as well if a concurrent lower eyelid repositioning is needed as well. I prefer to use small titanium microscrews or fixation of the implant along the infraorbital rim and cheek so that it lays completely flat along all bone surfaces.
Even with the use of a custom implant in vertical orbital dystopia it is important to realize that it is likely that some secondary adjustments of the eyelids or eyebrows may be needed. It is not known in ay case how the soft tissues will respond to a more complete orbitofacial skeletal correction.
Dr. Barry Eppley
Indianapolis, Indiana