

 Brow bone reduction is a very successful reshaping surgery of the forehead. It is most commonly done in two types of patients, the male with large overgrown brow one protrusions who wants to look more normal and the transgender male to female patient who is interested in a gender appearance change. Despite the disparate aesthetic goals, what they share is in how the procedure is performed.
Brow bone reduction is a very successful reshaping surgery of the forehead. It is most commonly done in two types of patients, the male with large overgrown brow one protrusions who wants to look more normal and the transgender male to female patient who is interested in a gender appearance change. Despite the disparate aesthetic goals, what they share is in how the procedure is performed.

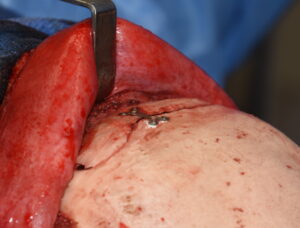
 The most significant brow bone reduction procedure involves a bone flap technique. This involves the removal of the bony cover (flap) of the frontal sinus, complete remodeling of the removed bone flap into a flatter shape and replacement over the exposed frontal sinus. This produces a far more effective brow bone reduction than simple burring alone could ever accomplish.
The most significant brow bone reduction procedure involves a bone flap technique. This involves the removal of the bony cover (flap) of the frontal sinus, complete remodeling of the removed bone flap into a flatter shape and replacement over the exposed frontal sinus. This produces a far more effective brow bone reduction than simple burring alone could ever accomplish.

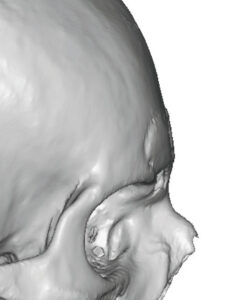
 While the bone flap brow bone reduction technique is widely used and successful, it is in some ways a remarkable procedure. This bone flap is reshaped by burring of its internal and external surfaces and then is put back where the only bone it contacts is around its perimeter. Much of the surface of this very thin bone is suspended over the frontal sinus where it continuously contacts contaminated air. Its only source of blood supply to re-establish vitality is from the overlying scalp on its outer surface.
While the bone flap brow bone reduction technique is widely used and successful, it is in some ways a remarkable procedure. This bone flap is reshaped by burring of its internal and external surfaces and then is put back where the only bone it contacts is around its perimeter. Much of the surface of this very thin bone is suspended over the frontal sinus where it continuously contacts contaminated air. Its only source of blood supply to re-establish vitality is from the overlying scalp on its outer surface.
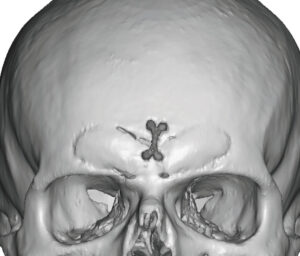
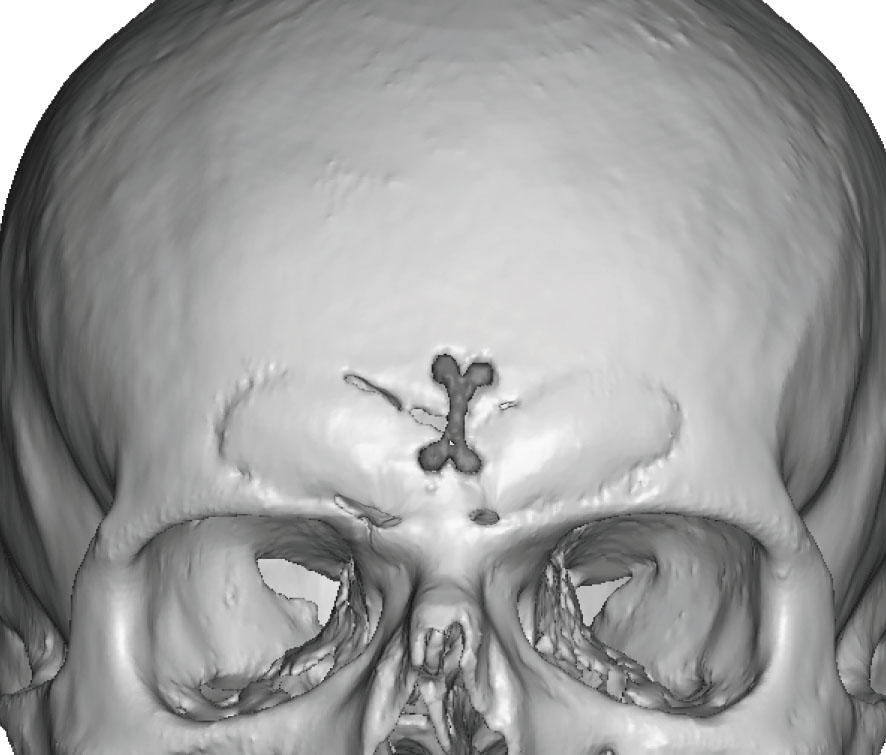
 What is remarkable is that any of the bone survives at all being so thin and having limited access to vascularized tissues. In theory all the bone should resorb…but yet it doesn’t. I have seen many 3D CT scans of healed bone flaps from brow bone reductions and most have good circumferential healing along the edges. It is common to see a few small areas at the perimeter where fibrous tissue rather than complete bone healing has occurred. But on a percentage basis this is relatively small.
What is remarkable is that any of the bone survives at all being so thin and having limited access to vascularized tissues. In theory all the bone should resorb…but yet it doesn’t. I have seen many 3D CT scans of healed bone flaps from brow bone reductions and most have good circumferential healing along the edges. It is common to see a few small areas at the perimeter where fibrous tissue rather than complete bone healing has occurred. But on a percentage basis this is relatively small.
While some may draw the corollary from bone healing over the maxillary sinus after LeFort surgery, this is not a good comparison. This is because this is an osteotomy line where the maxillary sinus bone above and below the osteotomy remains attached to well vascularized bone. (this is not a true bone flap)
 The explanation may be that the bone flap itself is not particularly well vascularized initially. Thus it can tolerate being extirpated and replaced without significant bone volume loss. But it also speaks to what can happen should infection occur. Its limited blood supply makes its resistance to infection as poor and with near complete resorption.
The explanation may be that the bone flap itself is not particularly well vascularized initially. Thus it can tolerate being extirpated and replaced without significant bone volume loss. But it also speaks to what can happen should infection occur. Its limited blood supply makes its resistance to infection as poor and with near complete resorption.
Dr. Barry Eppley
Indianapolis, Indiana