


In correction of the congenital webbed neck deformity, a posterior approach is used. Skin is excised and tightened in the midline which helps pull the neck webs more inward. But the neck webs also contain trapezius muscle fibers which are helpful to release to get a better result as well as to help prevent relapse.
But in the vicinity of the lateral border of the trapezius muscle lies the distal course of the spinal accessory nerve. Emerging from the posterior border of the sternocleidomastoid muscle it crosses the posterior triangle of the neck to supply motor innervation to the trapezius muscle. When considering trapezius muscle release in webbed neck surgery it is extremely pertinent to know where exactly the spinal accessory nerve is in relation to the muscle as injury to the nerve can result in shoulder dysfunction through scapular winging.
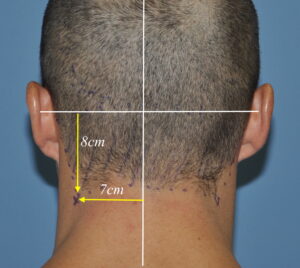 In the September 2020 issue of Plastic and Reconstructive Surgery an article was published entitled ‘In-Depth Look at the Anatomical Relationship of the Lesser Occipital Nerve, Greater Auricular Nerve, and Spinal Accessory Nerve and Their Implication in Safety of Operations in the Posterior Triangle of the Neck’. In this paper the authors performed an anatomic dissection where these three nerves were dissected out and measured compared to vertical and horizontal axises. The point of emergence of the spinal accessory nerve was determined to be 7.2cms lateral to the midline axis and 7.7cms inferior to the horizontal axis line.
In the September 2020 issue of Plastic and Reconstructive Surgery an article was published entitled ‘In-Depth Look at the Anatomical Relationship of the Lesser Occipital Nerve, Greater Auricular Nerve, and Spinal Accessory Nerve and Their Implication in Safety of Operations in the Posterior Triangle of the Neck’. In this paper the authors performed an anatomic dissection where these three nerves were dissected out and measured compared to vertical and horizontal axises. The point of emergence of the spinal accessory nerve was determined to be 7.2cms lateral to the midline axis and 7.7cms inferior to the horizontal axis line.

 While this anatomic study was done from the perspective of migraine surgery, it is just as relevant to webbed neck correction if lateral border trapezius muscle resection is to be performed. The goal is to release the muscle well below where the location of the spinal accessory nerve is to the outer border of the muscle. While there are various skin excisional patterns in webbed neck surgery, it is the lowest point along the web where the muscle should be released. Based on this anatomic study that appears to be well below where the nerve location is.
While this anatomic study was done from the perspective of migraine surgery, it is just as relevant to webbed neck correction if lateral border trapezius muscle resection is to be performed. The goal is to release the muscle well below where the location of the spinal accessory nerve is to the outer border of the muscle. While there are various skin excisional patterns in webbed neck surgery, it is the lowest point along the web where the muscle should be released. Based on this anatomic study that appears to be well below where the nerve location is.
 It is important to recognize, however, that the anatomy of the webbed neck patient may be different. The location of the hairline is well known to be lower than normal with even hair going down along the upper part of the webs. Does this mean that the location of the spinal accessory nerve is also lower? This can only be speculated that it might.
It is important to recognize, however, that the anatomy of the webbed neck patient may be different. The location of the hairline is well known to be lower than normal with even hair going down along the upper part of the webs. Does this mean that the location of the spinal accessory nerve is also lower? This can only be speculated that it might.
Dr. Barry Eppley
Indianapolis, Indiana