

Getting more defined cheekbones in either men or women can be challenging. In some patients they have decent cheekbone structure but their face is too full to show them well. In these cases facial defatting (buccal lipectomies, perioral liposuction) is often done to reduce the fullness below the cheekbones. In others they may have a thinner face but lack adequate cheekbone structure. Some form of structural cheekbone augmentation is then needed. (cheek implants, zygomatic sandwich osteotomy)
But for other patients it is really a combination of cheekbone augmentation and facial defatting that is needed. And for those that seek really defined cheeks it is almost always the diametric effects of bone augmentation and fat reduction that is required. Creating the classic Ogee curve requires increased convexity over the cheekbones as well as an increased concavity over the soft tissues of the cheek.
When augmenting the cheekbone structure for higher defined cheeks there is no standard implant that is deigned to create it. Standard cheek implants are oval in form and are made to provide fullness to the anterolateral malar-submalar areas. This creates more of a rounded effect to the cheeks, which may be fine for some women (not men) but would never be interpreted as a high cheekbone look. It simply doesn’t create the right cheek shape.
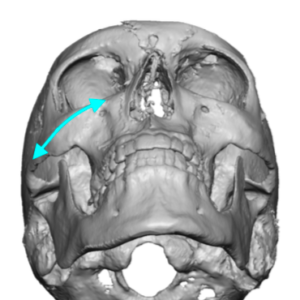
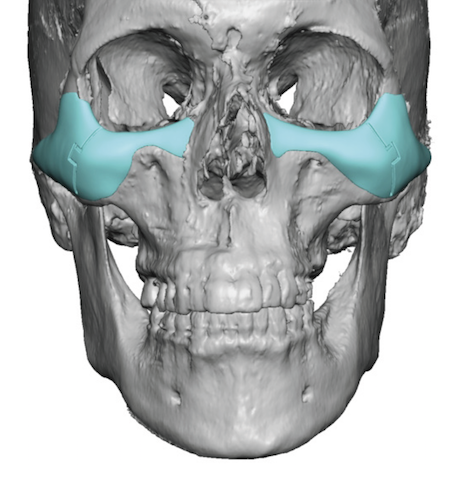
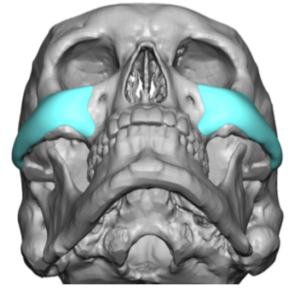
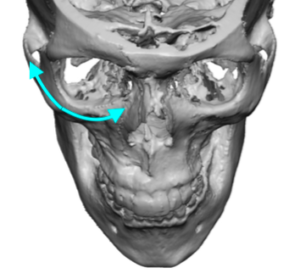 The high cheekbone look is, in many ways, exactly as it implies. The skeletal augmentation is a linear line along the cheekbone. The cheekbone is anatomically defined as the zygomatico-orbital complex. To effectively augment it there must be some extension anteriorly towards the infraorbital rim as well as posteriorly along the zygomatic arch. In essence the high cheekbone looks requires an augmentation that follows the natural shape of the bone. Only a custom cheek implant design can do so, not a standard cheek implant shape. Standard cheek implant put the fullness more toward the soft tissue of the cheek and not just isolated to bone coverage only.
The high cheekbone look is, in many ways, exactly as it implies. The skeletal augmentation is a linear line along the cheekbone. The cheekbone is anatomically defined as the zygomatico-orbital complex. To effectively augment it there must be some extension anteriorly towards the infraorbital rim as well as posteriorly along the zygomatic arch. In essence the high cheekbone looks requires an augmentation that follows the natural shape of the bone. Only a custom cheek implant design can do so, not a standard cheek implant shape. Standard cheek implant put the fullness more toward the soft tissue of the cheek and not just isolated to bone coverage only.
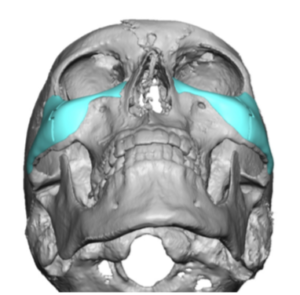 Such custom cheek implant designs can take on many iterations of these extensions. (differing lengths and thicknesses of coverage) Some may have a more complete infraorbital extension to simultaneously treat undereye hollows as well. Such infraorbital-malar cheek implant styles are best placed through a lower eyelid incision. They may even incorporate a geometric split design so they can sectioned for insertion through the small eyelid incision and then reassembled once inside the pocket.
Such custom cheek implant designs can take on many iterations of these extensions. (differing lengths and thicknesses of coverage) Some may have a more complete infraorbital extension to simultaneously treat undereye hollows as well. Such infraorbital-malar cheek implant styles are best placed through a lower eyelid incision. They may even incorporate a geometric split design so they can sectioned for insertion through the small eyelid incision and then reassembled once inside the pocket.
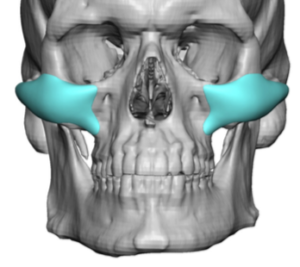
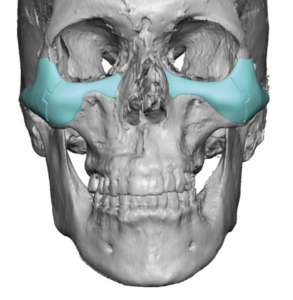
 Other cheek implant designs may have only a very limited infraorbital extension whose only purpose is to make the implant blend better into the eye area. This type of custom cheek implant is for the patient who does not have undereye hollows or has them only to a mild degree and does not choose to treat them. This type of custom cheek implant can be placed through an intraoral approach right up under the upper lip.
Other cheek implant designs may have only a very limited infraorbital extension whose only purpose is to make the implant blend better into the eye area. This type of custom cheek implant is for the patient who does not have undereye hollows or has them only to a mild degree and does not choose to treat them. This type of custom cheek implant can be placed through an intraoral approach right up under the upper lip.

 Regardless of the design of the high cheekbone look implant, facial defatting is almost always beneficial. Whether it is buccal lipectomies alone or combined with perioral liposuction depends on the patient’s facial shape. In less full faces a buccal lipectomy alone may suffice. But in fuller faces maximal facial defatting is needed which must include the lower perioral region as well.
Regardless of the design of the high cheekbone look implant, facial defatting is almost always beneficial. Whether it is buccal lipectomies alone or combined with perioral liposuction depends on the patient’s facial shape. In less full faces a buccal lipectomy alone may suffice. But in fuller faces maximal facial defatting is needed which must include the lower perioral region as well.
The high cheekbone look often requires a dual approach to try and achieve. It is not a facial look that is easily obtained in many patients and is why a the combined augmentation-reduction approach is needed.
Dr. Barry Eppley
Indianapolis, Indiana