


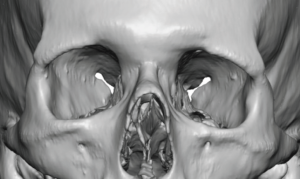
Background: There are many causes of eye asymmetry due to the numerous structures that surround the eyeball from the eyelids, brow bone, and the eyebrow. These make up the most common causes of eye asymmetry. The one unique causes of eye asymmetry is that of the eyeball itself. This is when the eyeball on one side is different in either the horizontal, vertical or both axes. This is known as orbital dystopia can be caused by natural developmental differences, trauma with loss of orbital floor support and tumors causing displacement.
One of the most common orbital dystopias is vertical where the involved eye sits lower from a congenital origin. Typical aesthetic vertical orbital dystopia (VOD) is usually mild by dystopia standards being less than 5mm as measured by a horizontal pupillary line from the normal or higher eye. I have chosen to use the term aesthetic because this indicates that it is possible to treat it effectively without doing orbital box osteotomies.
The cornerstone of aesthetic VOD surgery is the bony elevation of the lower orbital floor and infraorbital rim using a custom designed implant. But that alone is not enough as raising the eye by itself displaced it from the surrounding soft tissues which were established for when the eye was lower. As a result you can’t just move the eye without changing everything around it.
 Case Study: This male had left VOD of 4mms with typical lower eyelids, eyebrow and brow bone asymmetry associated with it. His surgical plan and execution consisted of the following six procedures:
Case Study: This male had left VOD of 4mms with typical lower eyelids, eyebrow and brow bone asymmetry associated with it. His surgical plan and execution consisted of the following six procedures:
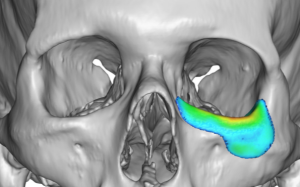
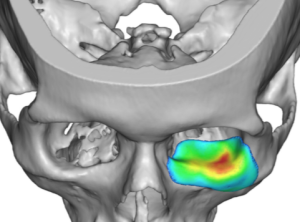

 Placement of a custom left orbital floor-rim implant through a lower eyelid approach. to raise up the lower orbital box bone.
Placement of a custom left orbital floor-rim implant through a lower eyelid approach. to raise up the lower orbital box bone.
 A drill hole lateral canthoplasty done through an upper eyelid incision.
A drill hole lateral canthoplasty done through an upper eyelid incision.
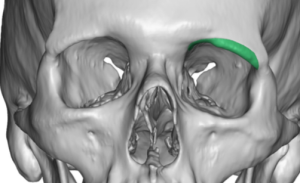 A left inferior brow bone reduction for the low hanging bottom edge of the upper orbital box bone.
A left inferior brow bone reduction for the low hanging bottom edge of the upper orbital box bone.
 A direct browlift done through the upper eyelid using screw fixation.
A direct browlift done through the upper eyelid using screw fixation.
![]() An Alloderm spacer graft to the lower eyelid to help support its elevated position that works in tandem with the lateral canthoplasty.
An Alloderm spacer graft to the lower eyelid to help support its elevated position that works in tandem with the lateral canthoplasty.
 An upper eyelid ptosis repair with upper eyelid closure was done last.
An upper eyelid ptosis repair with upper eyelid closure was done last.

 As one might imagine this much work around the eye causes a lot of swelling that takes a full 6 to 8 weeks to truly see its final effects. His postoperative result showed good correction with a remaining mild upper eyelid ptosis.
As one might imagine this much work around the eye causes a lot of swelling that takes a full 6 to 8 weeks to truly see its final effects. His postoperative result showed good correction with a remaining mild upper eyelid ptosis.
This six step vertical orbital dystopia correction approach fully addresses every associated component of the problem. Not all VOD patients will need every step but, conversely, it would be rare to ever need just one. (the orbital implant) The least predictable of the procedures are that of the eyelids, particularly getting the level of the upper eyelid to the iris at a symmetric level. Raising the eye creates an intraoperative upper eyelid ptosis that usually did not exist before. As the last part of the VOD procedure it is the least predictable step as how much the upper eyelid should be elevated is but a guess in these intraoperative circumstances. For this reason a secondary upper lid ptosis correction/refinement is frequently needed.
Case Highlights:
1) Aesthetic vertical orbital dystopia is when the horizontal pupillary line difference between the two eyes is 5mms or less.
2) While a custom orbital floor-rim implant is a foundational element of VOD repair, it requires treatment of all the surrounding soft tissue structures as well.
3) The most common reason for VOD surgery revision is for upper eyelid ptosis repair.
Dr. Barry Eppley
Indianapolis, Indiana