


Background: Surgery of the bony jaw angles is unique from other parts of the lower jaw due to the large masseter muscle that lies over it. The posterior-inferior border of the jaw angles serve as the focused insertion point of the masseter muscle from its broad origin along the zygomatic body and arch. This insertion area is very relevant it has strong ligamentous attachments since it is what the muscle moves. This is very different from the mentalis muscle of the chin where the insertion of the muscle is not on the lower chin bone but out onto the more superficial soft tissues.
All surgical procedures of the jaw angles requires elevation of the bulk of the muscle in the bony recess above its posterior and inferior borders. Depending upon the procedure the insertion area directly over the angle may require elevation of varying degrees. But when an implant is being used to augment the jaw angles the ligamentous insertions always need to be lift off from the bone. This is particularly relevant when there is any amount of vertical lengthening required by the implant.
With elevation of the masseter muscle ligaments from the jaw angles there is always the risk the muscle will retract superiorly (away from the jaw angles) after surgery. That risk is enhanced with an implant because of its volumetric displacement, pushing the overlying muscle away from the bone. Without a firm insertion attachment the muscle retracts up along the ramus of the jaw angles creating a distinct oblique line. (now the new insertion area of the muscle) This is known as masseteric muscle dehiscence (MMD) and is almost always described with implants and very rarely with bone surgery.
MMD creates a soft tissue contour deformity over the jaw angles but does not cause any negative impact on jaw motion/function. It is a pure aesthetic soft tissue deficiency (lack of muscle) over the jaw angles now having only skin, fat, and implant capsule and an implant next to the bone. It is largely seen when chewing or biting down which creates an abnormal bulge higher up along the side of the jawline.
While the anatomic basis for MMD is easy to understand, how to successfully treat it is not so easy. The anatomic approach is to try and pull the muscle back down over the implant. Besides requiring an external skin incision and scar in the neck below the jaw angles it is also a procedure that does not have a high rate of success. This is not to say that it never works but it is far from an assured procedure whose success rate is influenced by its severity and the length of time from the initial implant surgery.
The alternative approach is a camouflage one, creating soft tissue augmentation effect. This can be done by injectable fillers, fat injections, allograft dermis, dermal-fat grafts and even implants. When using implants, a seemingly unlikely option, the key is to make it for its intended purpose…a soft tissue and not a bony implant.
Case Study: This male had significant MMD from prior jaw implant surgery. Once his jaw angle implants were improved he had a very significant jaw angle soft tissue contour deformity. He had an initial set of custom soft tissue jaw angle implants which provided a remarkable contour improvement. He returned wanting larger soft tissue jaw angle implants for an even better result.

 His initial markings showed the surface area coverage of the new soft tissue jaw angle implants, the largest I have yet done.
His initial markings showed the surface area coverage of the new soft tissue jaw angle implants, the largest I have yet done.
 Under general anesthesia and through his existing external well healed jaw angle incisions the indwelling soft tissue jaw angle implants were removed by opening up their posterior capsule. In comparing the removed implants with their replacement the increased surface area coverage could be easily seen.
Under general anesthesia and through his existing external well healed jaw angle incisions the indwelling soft tissue jaw angle implants were removed by opening up their posterior capsule. In comparing the removed implants with their replacement the increased surface area coverage could be easily seen.
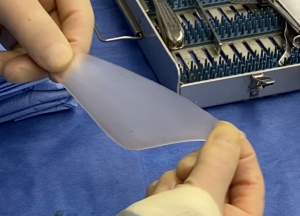
 The new larger soft tissue jaw angle implants were made of an ultrasoft silicone implant material made to feel like muscle not bone.
The new larger soft tissue jaw angle implants were made of an ultrasoft silicone implant material made to feel like muscle not bone.

 To add to the soft tissue thickness over the jaw angles a new subcapsular pocket was developed for the new implants. This also added an additional layer of soft tissue for a more reinforced closure.
To add to the soft tissue thickness over the jaw angles a new subcapsular pocket was developed for the new implants. This also added an additional layer of soft tissue for a more reinforced closure.

![]() For the properly selected patient and in seeking a permanent augmentation solution to lack of implant muscle coverage, a soft tissue jaw angle implant can be effective. The concept of a soft tissue implant to replicate muscle is not new in the face. It is the same concept that is used for temporal augmentation. The only difference between the two is that the temporal implant are placed subfascial while the massteric muscle implant is subcutaneous…because there is not muscle there. The surface coverage of the soft tissue jaw angle implant is like a right and left angle triangle using the posterior (altitude) and inferior bony border (base) of the bony jaw angle and its superior border (hypotenuse) extends just beyond the inferior border of the muscle dehiscence.
For the properly selected patient and in seeking a permanent augmentation solution to lack of implant muscle coverage, a soft tissue jaw angle implant can be effective. The concept of a soft tissue implant to replicate muscle is not new in the face. It is the same concept that is used for temporal augmentation. The only difference between the two is that the temporal implant are placed subfascial while the massteric muscle implant is subcutaneous…because there is not muscle there. The surface coverage of the soft tissue jaw angle implant is like a right and left angle triangle using the posterior (altitude) and inferior bony border (base) of the bony jaw angle and its superior border (hypotenuse) extends just beyond the inferior border of the muscle dehiscence.
Case Highlights:
1) Masseteric muscle dehiscence (MMD) is a potential risk in any jaw angle surgery which is greatest in implant augmentation.creates a soft tissue contour deformity at the jaw angles
2) MMD is an aesthetic soft tissue contour deformity at the jaw angles with lack of muscle over the implant.
3) One technique for improving the soft tissue contour deformity of MMD is a camouflage approach with the subcutaneous placement of an ultrasoft silicone implant.
4) A second stage larger soft tissue jaw angle implant can be placed beneath the capsule of the indwelling soft tissue implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon