

Background: The shape of the lower ribcage is created by the union of the cartilaginous components of the false ribs as they wrap around the side of the lower chest and merge into the sternum. These cartilaginous rib lengths and how they merge together creates a lot of variation in the costal margins. The costal margin is well known to be affected in chest well deformities, such as pectus excavatum and pectus carinatum, where the ribs and the costal margin either on one or both sides are pulled upwards and stick out. (rib flaring) But rib flaring or winged ribs is far more commonly seen in isolation with no associated chest wall deformities.
Many cases of rib flare are posturally related. It can occur with a posture that causes the lower ribs to protrude forward and is usually accompanied by breastbone elevation. This is correctable by physiotherapy alone. But rib flare that is structurally based with a normal posture is correctable only by some form of cartilage reshaping/modification. This comes down to two fundamental chondroplasty approaches, rib excision/removal or rib bending/reshaping.
Cartilage removal of rib protrusions of #10, #9 and #8 is done by a small subcostal incision. Due to the location of the pleura of the lung rib removals above #8 have increased risk and external shaving of their outer surface is safer. Rib shaving can be done without removal but a combination of both is usually the most effective. Rib bending is done by weakening of the costochondral junction laterally and a second cut more medially. It relies on the pressure of postoperative banding to move the partially mobilized subcostal flare inward where it can heal and overcome any rib memory. It can the done with open and percutaneous techniques of which currently it is unclear if one approach is better than the other or even if they have similar results.
 Case Study: This female presented with subcostal margin prominences with the left being much more pronounced than the right. This has long been of a concern to her and left side caused some discomfort when laying on it. The right costal margin showed a modest and typical rib flare but the left side has a very pronounced subcostal bulge that was atypical for rib flare.
Case Study: This female presented with subcostal margin prominences with the left being much more pronounced than the right. This has long been of a concern to her and left side caused some discomfort when laying on it. The right costal margin showed a modest and typical rib flare but the left side has a very pronounced subcostal bulge that was atypical for rib flare.

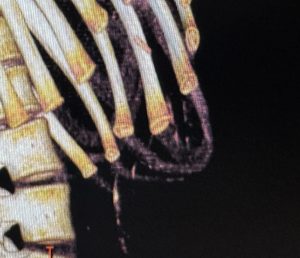
 A 3D CT scan of her ribcage showed significant hypoplasia of ribs #12. They were quite small and were easy to miss. But rib counting from the top showed that these nubs were hypoplasic #12 ribs.
A 3D CT scan of her ribcage showed significant hypoplasia of ribs #12. They were quite small and were easy to miss. But rib counting from the top showed that these nubs were hypoplasic #12 ribs.

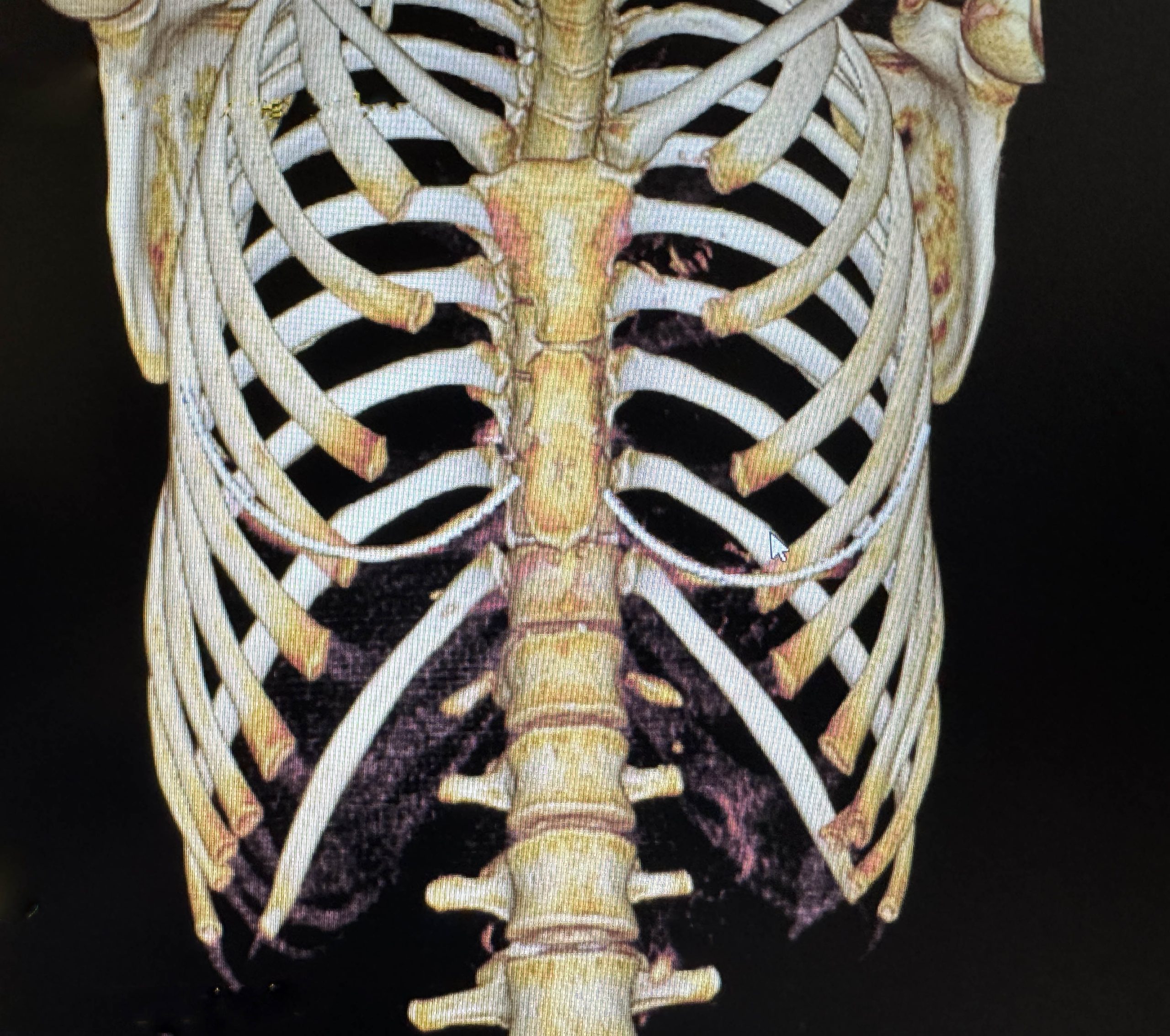
 The costal margins looked quite different with the right side cartilages looking normal with a modest flare. But the left side showed a confluence of cartilages that was bent and twisted with increased density/bulging. The bony ribs didn’t look much different between the two sides.
The costal margins looked quite different with the right side cartilages looking normal with a modest flare. But the left side showed a confluence of cartilages that was bent and twisted with increased density/bulging. The bony ribs didn’t look much different between the two sides.
 Looking at the 2D slicing the abnormal bending/twisting of the left costal cartilages causing the left chest wall bulge could be appreciated.
Looking at the 2D slicing the abnormal bending/twisting of the left costal cartilages causing the left chest wall bulge could be appreciated.

 Under general anesthesia and in the supine where the abdomen is fully relaxed the magnitude of the left subcostal protrusion deformity could be fully appreciated.
Under general anesthesia and in the supine where the abdomen is fully relaxed the magnitude of the left subcostal protrusion deformity could be fully appreciated.

 Initially the left side was approached through a 4cm incision in a high abdominal wrinkle line near/over the subcostal margin.Through this incision the cartilaginous ends of rib #9 and 10 were removed. Rib #8 was extensively shaved down as far medially as the incision would permit. To get more flare/bulge reduction a medial and lateral cut was made in rib # 8 to allow it to bent inward. This then allowed some shaving reduction of rib #7. A large amount of costal cartilage was removed along with the inward bending of the remaining rib #8.
Initially the left side was approached through a 4cm incision in a high abdominal wrinkle line near/over the subcostal margin.Through this incision the cartilaginous ends of rib #9 and 10 were removed. Rib #8 was extensively shaved down as far medially as the incision would permit. To get more flare/bulge reduction a medial and lateral cut was made in rib # 8 to allow it to bent inward. This then allowed some shaving reduction of rib #7. A large amount of costal cartilage was removed along with the inward bending of the remaining rib #8.
 On the opposite right side with a more normal flare of the cartlages which had a far less protrusion than the left, medial and lateral cuts of rib#8 were only done whose effect would require postoperative banding.
On the opposite right side with a more normal flare of the cartlages which had a far less protrusion than the left, medial and lateral cuts of rib#8 were only done whose effect would require postoperative banding.

 The incisions were closed in multiple layers with resorbable sutures after the placement of Exparel-soaked Gelfoam sponges for postoperative pain relief. Her intraoperative supine results show a substantial reduction in the deformed left subcostal protrusion and no results yet in the right subcostal rib flare.
The incisions were closed in multiple layers with resorbable sutures after the placement of Exparel-soaked Gelfoam sponges for postoperative pain relief. Her intraoperative supine results show a substantial reduction in the deformed left subcostal protrusion and no results yet in the right subcostal rib flare.
While a subcostal rib flare is not uncommon a subcostal cartilaginous ribcage deformity is. A preoperative 3D CT scan is essential to understand the ribcage anatomy and the source of the subcostal deformities seen. There are a variety of cartilage reshaping techniques from excision, shaving to bending. Each technique has its place and in this patient all three were necessary given the different origins of the deformity.
Key Points
1) Subcostal flare and a subcostal deformity are different anterior lower ribcage issues that are treated differently. This patient example has both.
2) An abnormal subcostal protrusion is part of an overall ribcage deformity that Is a collection of anomalous cartilage overgrowths for which excision reduction is the primary treatment method.
3) Subcostal flare is the excessive projection of the lower ribcage which can be treated in some cases with cartilage weakening and postoperative banding for its reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon