

Background: The prominence of the brow bones is largely a reflection of the size of the underlying frontal sinus cavities. The frontal sinus is technically composed of four pairs of paranasal sinuses which are mucosal lined and drain into the nose through the frontonasal duct. While absent after birth and the first few years thereafter, they develop into a well defined structure by childhood and reach their full size after puberty. Men are well known to have larger frontal sinuses than women which is primary seen near the midline. Like the size of the skull between men and women these differences are rimarily due to genetic factors.
Because of the genetic differences men are much more prone to develop brow bone hypertrophy or over aeration of the frontal sinuses. They can become quite enlarged and develop a ‘Neanderthal’ appearance which causes undesirable appearance and expression issues. Because of the thickness of the anterior table of the frontal sinus and the amount of brow bone reduction needed, burring of the anterior table to achieve a reduction will be inadequate. With the average anterior table thickness in men of around 4mms and significant reduction needed of 10+ mms, only a bone flap brow bone reduction technique can be aesthetically successful.
The male forehead has a more acute nasofrontal angle and steeper posterior forehead inclination than women. The glabella in men is also wider and more frequently protrudes beyond the ideal forehead slope line. For these anatomic reasons the addition of forehead augmentation to the brow bone reduction procedure in men is often needed to get a visible brow bone reduction that flows more naturally up into the forehead. It also prevents the possibility if a central over reduction of the brows, which will beneficial in male to female transgender brow bone reduction procedures is not aesthetically desirable in men.
Case Study: This older male had a near lifelong concern about his severe brow bone protrusion. His overall vertical forehead length was short and it had a significant indentation along the suprabrow bone break.

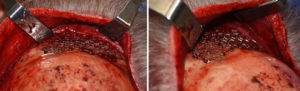
 Under general anesthesia and through a near complete coronal scalp incision the forehead was widely exposed down over the brow bones in the subperiosteal plane. The external shape of the forehead and brows could be seen on the bone with a brow bone protrusion and a forehead deficiency. In doing the dissection the supraorbital neurovascular bundle was preserved.
Under general anesthesia and through a near complete coronal scalp incision the forehead was widely exposed down over the brow bones in the subperiosteal plane. The external shape of the forehead and brows could be seen on the bone with a brow bone protrusion and a forehead deficiency. In doing the dissection the supraorbital neurovascular bundle was preserved.

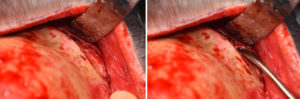
 A reciprocating saw was used to remove the protruding brow bones exposing the large underlying frontal sinuses. Very thick mucosal lining was then removed down to the frontonasal duct.
A reciprocating saw was used to remove the protruding brow bones exposing the large underlying frontal sinuses. Very thick mucosal lining was then removed down to the frontonasal duct.

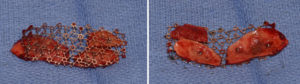
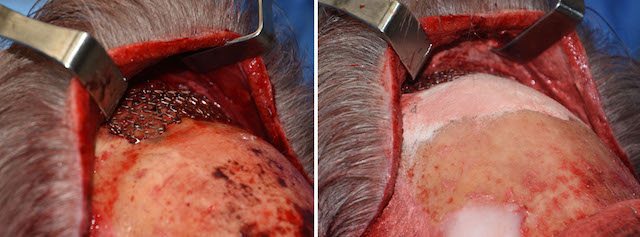
 Due to the size of the anterior table defects and the curved shape of the removed brow bones, extra bone was needed. A split-thickness cranial bone graft was harvested from behind the left coronal suture line. The outer contour was restored with bone wax.The anterior table defect was reconstructed by putting the brow bone pieces, including the cranial bone graft, onto a mesh screen with small screws whose perimeter was bigger than the brow bone defect over which it was placed.
Due to the size of the anterior table defects and the curved shape of the removed brow bones, extra bone was needed. A split-thickness cranial bone graft was harvested from behind the left coronal suture line. The outer contour was restored with bone wax.The anterior table defect was reconstructed by putting the brow bone pieces, including the cranial bone graft, onto a mesh screen with small screws whose perimeter was bigger than the brow bone defect over which it was placed.

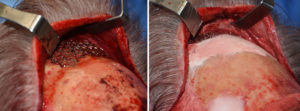 Hydroxyapatite cement (15ccs) was then used to fill in the horizontal suprabrow bone break and upper forehead defect. Its inferior edge blended into the upper portion of the mesh fixation plate.
Hydroxyapatite cement (15ccs) was then used to fill in the horizontal suprabrow bone break and upper forehead defect. Its inferior edge blended into the upper portion of the mesh fixation plate.
It should be determined before surgery whether concomitant forehead augmentation is of benefit. If so bone cement is an effective procedure when done in conjunction with brow bone reduction. While the use of PMMA bone cement must be used with caution and keep away from the brow bone area, hydroxyapatite can be used up to and over a position of it.
Case Highlights:
1) Male brow bone reduction always requites a bone flap setback technique.
2) Males often have a backward slope to the forehead which magnified the appearance of protruding brows.
3) Bone cement forehead augmentation combined with brow bone reduction creates a more pleasing forehead shape than either one alone in many men.
Dr. Barry Eppley
Indianapolis, Indiana