


Background: The gummy smile is a well known aesthetic oral deformity where excessive gum show appears when smiling. The accepted amount of gum show when smiling is 1 to 2mms at most. Such gummy smile appearances can occur for two reasons, excessive maxillary vertical length and/or a hyperdynamic smile motion. (excessive upper lip pull)
Vertical maxillary excess exists when upper tooth show exists when the lips are at rest. With a longer maxilla the upper and lower lips do not meet at rest or only do so with some lip strain. When smiling the entire upper teeth and considerable gum show occurs. When considerable tooth show is present a maxillary or LeFort I impaction would be the corrective procedure. If the tooth show is more minor (1 or 2mms) then correction of only the gummy smile can be done.
With a normal maxillary position, a gummy smile occurs due to over activity/excessive pull of the lip elevators muscles particularly the levator anguli oris and levator labii superioris. This can be very effectively treated non-surgically by Botox injections albeit not permanently. A more permanent method is surgical by altering the depth/shape of the vestibule.
The vestibule is the space between the teeth and the lips/cheek. When the upper lip elevates during smiling part of its excursion capability is due to the presence and depth of the vestibule. Interestingly in my observation many gummy smile patients have ‘high’ vestibules which allows for a lot of excursion of the upper lip. Shortening or lowering of the vestibular depth creates a limitation or stop of the amount of upper lip movement when smiling.
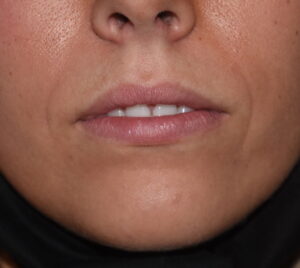
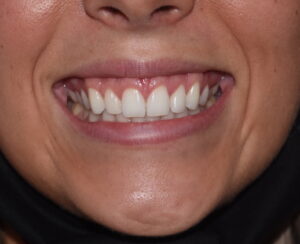 Case Study: This female had a gummy smile with several millimeters of tooth show at rest and 7mms of gingival show at maximum smile. The tooth show at rest indicates that there was some element of vertical maxillary excess. But with prior orthodontic therapy the magnitude of the maxillary excess did not justify an upper jaw shortening procedure.
Case Study: This female had a gummy smile with several millimeters of tooth show at rest and 7mms of gingival show at maximum smile. The tooth show at rest indicates that there was some element of vertical maxillary excess. But with prior orthodontic therapy the magnitude of the maxillary excess did not justify an upper jaw shortening procedure.
 The depth of her maxillary vestibule at the level of the lateral incisors was 17mms.
The depth of her maxillary vestibule at the level of the lateral incisors was 17mms.

 Under local anesthesia a 10mm wedge of mucosa was removed from several millimeters above the mucogingoval line and onto the upper lip mucosa. Electrocautery dissection was done superiorly into the paranasal areas where levator myotomes were performed.
Under local anesthesia a 10mm wedge of mucosa was removed from several millimeters above the mucogingoval line and onto the upper lip mucosa. Electrocautery dissection was done superiorly into the paranasal areas where levator myotomes were performed.
 The edge of the upper lip mucosa was then sewn down to the maxillary mucogingival cuff of tissue.
The edge of the upper lip mucosa was then sewn down to the maxillary mucogingival cuff of tissue.

 Her immediate result show substantial reduction in her gummy smile appearance.
Her immediate result show substantial reduction in her gummy smile appearance.
 A lowering vestibuloplasty is the primary procedure for gummy smiles due to hyperdynamic smile muscle motion. Levator myotomes provide some additional benefit. In the patient with some tooth show at rest a central V-Y mucosal advancement can be done at the frenal attachment to also lengthen the upper lip.
A lowering vestibuloplasty is the primary procedure for gummy smiles due to hyperdynamic smile muscle motion. Levator myotomes provide some additional benefit. In the patient with some tooth show at rest a central V-Y mucosal advancement can be done at the frenal attachment to also lengthen the upper lip.
Case Highlights:
1) Gummy smiles are when more than 1mm of gingiva is seen with the lip lift during smiling and is often associated with vertically long intraoral vestibules.
2) Shortening the maxillary vestibule is an effective technique for decreasing the excursion of the upper lip during smiling.
3) If there is tooth show at rest between the upper and lower lips a V-Y mucosal advancement can be done centrally for some upper lip lengthening.
Dr. Barry Eppley
Indianapolis, Indiana