

Background: When evaluating facial asymmetries I divide them into two basic types, craniofacial and aesthetic. Some many view this distinction as minor vs major but the terms craniofacial and aesthetic is more meaningful as it differentiates how they are treated. Major facial asymmetries are often syndromic (e.g., hemifacial microsomia), usually involve earlier intervention in childhood and teen years and are treated using well known craniofacial reconstructive surgery techniques. In contrast aesthetic facial asymmetries are less dramatic in appearance, attempts at correction are not done until late teens or adulthood and they are treated by more aesthetic-based camouflage bone and soft tissue methods.
One specific type of congenital facial asymmetry is that of vertical orbital dystopia. (VOD) This is where the orbital box is positioned lower on one side which makes the horizontal position of the eyes different. VOD is very often part of an overall facial asymmetry and may be the most noticeable feature of it. But it can also occur as a pure isolated facial asymmetry. In more severe cases of VOD (greater than 5 or 6mms which I call craniofacial VOD) early efforts at repositioning the orbital box can be done. (frontal craniotomy/orbital osteotomies) But in aesthetic VOD (5mm or less of horizontal pupillary line asymmetry) cranofacial surgery techniques may often be viewed as a surgical approach that is bigger than the problem.
In treated aesthetic VOD, it is important to recognize that the problem is more than just the orbital floor being lower. The entire bony orbital box is lower (superior and infraorbital rims) as well as all overlying soft tissue that surrounds the eye is malpositioned. As a result in treating VOD each of the bony and soft tissue components must be addressed to get the best aesthetic result. These include the orbital floor/infraorbital rim/superior tail of the brow bone/cheekbone), upper and lower eyelids and the eyebrows. This creates a 6 step approach to the treatment of aesthetic VOD.

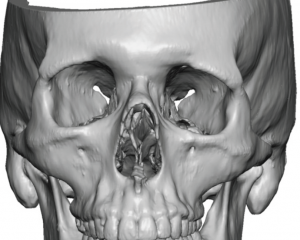 Case Study: This male had a left vertical orbital dystopia of 5mms. He had no visual acuity or double vision problems. A 3D CT scan showed the entire inferiorly displaced orbital box bone.
Case Study: This male had a left vertical orbital dystopia of 5mms. He had no visual acuity or double vision problems. A 3D CT scan showed the entire inferiorly displaced orbital box bone.
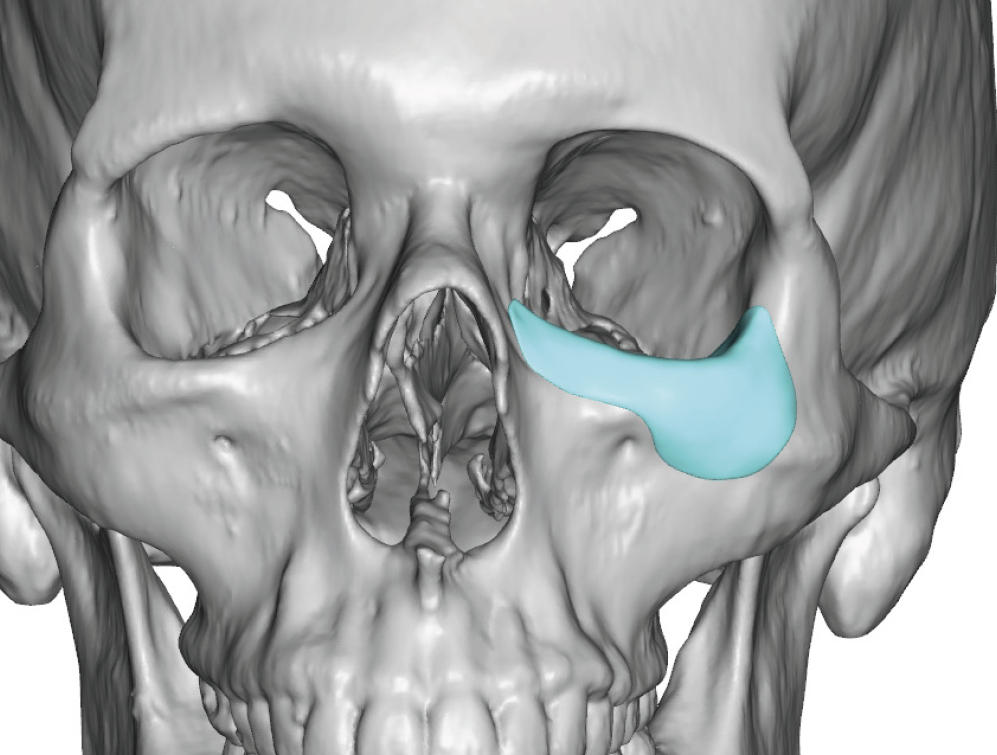
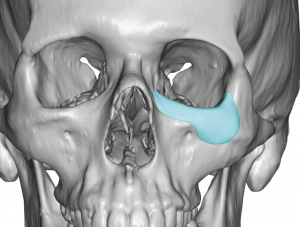 A custom orbital floor/rim/anterior cheek implant was designed by copying the normal right orbital box anatomy and making the implant replicate the difference between the two sides.
A custom orbital floor/rim/anterior cheek implant was designed by copying the normal right orbital box anatomy and making the implant replicate the difference between the two sides.


 Under general anesthesia Step 1 VOD correction was done by placing the implant through a lower eyelid incision (skin-muscle flap) and securing it to the infraorbital rim by microscrew fixation.
Under general anesthesia Step 1 VOD correction was done by placing the implant through a lower eyelid incision (skin-muscle flap) and securing it to the infraorbital rim by microscrew fixation.
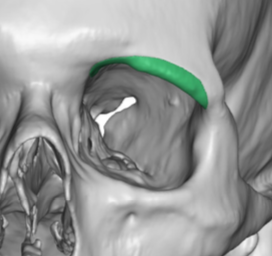
 Step 2 was removal of the low hanging inferior edge of the tail of the brow bone through an upper eyelid incision using a small high speed burr.
Step 2 was removal of the low hanging inferior edge of the tail of the brow bone through an upper eyelid incision using a small high speed burr.
 Step 3 was a lateral canthoplasty using a drill hole technique through the upper eyelid, placing the lateral canthus at the level of the fronto-zygomatic suture line.
Step 3 was a lateral canthoplasty using a drill hole technique through the upper eyelid, placing the lateral canthus at the level of the fronto-zygomatic suture line.
![]() Step 4 is an eyebrow lift. In this case of a young shaved head male any superior approach was not aesthetically advised. An inferior technique thorough the upper eyelid was done by wide subperiosteal undermining of the left eyebrow and forehead. The released periosteum along the inferior edge of the brow bone was sewn up to a small screw in the suprabrow area for a few millimeters of outer browlift.
Step 4 is an eyebrow lift. In this case of a young shaved head male any superior approach was not aesthetically advised. An inferior technique thorough the upper eyelid was done by wide subperiosteal undermining of the left eyebrow and forehead. The released periosteum along the inferior edge of the brow bone was sewn up to a small screw in the suprabrow area for a few millimeters of outer browlift.
Step 5 was an upper eyelid ‘ptosis’ repair of 2mms using three tarsal plate-levator sutures with a 2mm skin removal.
![]()
 Step 6 was placement of a spacer graft to the lower eyelid using Alloderm material.
Step 6 was placement of a spacer graft to the lower eyelid using Alloderm material.
 While some slight facial asymmetries are common, and we all have them, they are ascribed by many as a feature of natural beauty. But when they become more significant (and the interpretation of significant is very individually based) they are viewed as detracting from one’s facial appearance and often very bothersome to the patient. Aesthetic VOD falls into this category of one the most bothersome of adult facial asymmetries Using a comprehensive 6 step approach, aesthetic VOD facial asymmetries can be improved albeit perfect orbital/eye asymmetry will likely not be achieved. Not every VOD patients requires all six procedures to improve it and each patient must be individually assessed for what they need. Conversely it would not be likely than a custom orbital implant alone would be sufficient.
While some slight facial asymmetries are common, and we all have them, they are ascribed by many as a feature of natural beauty. But when they become more significant (and the interpretation of significant is very individually based) they are viewed as detracting from one’s facial appearance and often very bothersome to the patient. Aesthetic VOD falls into this category of one the most bothersome of adult facial asymmetries Using a comprehensive 6 step approach, aesthetic VOD facial asymmetries can be improved albeit perfect orbital/eye asymmetry will likely not be achieved. Not every VOD patients requires all six procedures to improve it and each patient must be individually assessed for what they need. Conversely it would not be likely than a custom orbital implant alone would be sufficient.
Case Highlights:
1) Aesthetic vertical orbital dystopias (VOD) have 5mms or less of horizontal pupillary line discrepancies.
2) The anterior orbital floor and eyeball can be safely raised up to 4 or 5mms using a custom designed orbital implant that replicates the opposite normal orbital anatomy.
3) The overlying eyelids and eyebrows must also be assessed to determine if their positioning needs to be elevated as well. If so some or all of the described six steps of VOD correction may be needed.
Dr. Barry Eppley
Indianapolis, Indiana