


Rib removal is a general but recognized term that applies to waistline narrowing surgery. On the surface the term would imply that rib removals are done and the waistline will fall further inward with the loss of outer bony support. While this is true it is not quite that simplistic. To provide a more in-depth understanding about the surgery it is helpful to clarify some basic concepts about it that explain how the surgery is done and how it anatomically works.
Rib Removal Is Often Done As Part Of Other Body Contouring Procedures

 On average about 2/3s of rib removal surgeries are part of a multi-procedure body contouring effort. The most common concomitant procedures are done from the same prone position (face down) and would be buttock augmentation (implant or BBL), hip augmentation (implants or fat injections) and liposuction. (flank liposuction is a part of rib removal surgery but other body areas can be done as well, e.g., back and chest wall) When numerous procedures around the waistline are done the overall waistline narrowing effect is improved because of their cumulative effect. This will, of course, prolong the recovery to some degree. Whether such combinations of procedures are done on any particular patient is preoperatively determined by a variety of factors including an assessment of the patient’s ability to safely undergo multiple procedures and what their postoperative support system is for their recovery period.
On average about 2/3s of rib removal surgeries are part of a multi-procedure body contouring effort. The most common concomitant procedures are done from the same prone position (face down) and would be buttock augmentation (implant or BBL), hip augmentation (implants or fat injections) and liposuction. (flank liposuction is a part of rib removal surgery but other body areas can be done as well, e.g., back and chest wall) When numerous procedures around the waistline are done the overall waistline narrowing effect is improved because of their cumulative effect. This will, of course, prolong the recovery to some degree. Whether such combinations of procedures are done on any particular patient is preoperatively determined by a variety of factors including an assessment of the patient’s ability to safely undergo multiple procedures and what their postoperative support system is for their recovery period.
Rib Removal Means A Resection Of the Outer Half Of The Ribs, Not The Whole Ribs
It is a common misconception that removal of the ribs for waistline narrowing means the whole ribs taken. This is not true nor would there ever be a need to do so. It is the outer 1/3 or 1/2 of the rib that is removed since this is what supports the outer waistline. Taking the whole rib would require disarticulating it from its vertebral attachment with the need for a considerably longer incision and a much higher risk of bleeding and nerve injury.
Rib Removal Is Done Using A Tunnel Delivery Technique



 Because it is the outer aspect of the ribs that are removed, it takes a small lateral incision to do so. In traditional thoracic surgery, for different reasons, any rib resection is done by making an incision almost as long as the section of the rib to be removed. There may be little regard for the intercostal neurovascular bundle located on the inferior edge of the rib. In aesthetic waistline narrowing surgery a small skin incision is made, just enough to make a proximal full-thickness cut through the rib where one wants the resection to begin. The now free end of the rib is then turned 90 degrees and slowly taken out of the incision as the soft tissue attachments are circumferentially released around it. In essence the rib is extracted through a narrow tunnel. This technique is tedious but keeps the incision as small as possible.
Because it is the outer aspect of the ribs that are removed, it takes a small lateral incision to do so. In traditional thoracic surgery, for different reasons, any rib resection is done by making an incision almost as long as the section of the rib to be removed. There may be little regard for the intercostal neurovascular bundle located on the inferior edge of the rib. In aesthetic waistline narrowing surgery a small skin incision is made, just enough to make a proximal full-thickness cut through the rib where one wants the resection to begin. The now free end of the rib is then turned 90 degrees and slowly taken out of the incision as the soft tissue attachments are circumferentially released around it. In essence the rib is extracted through a narrow tunnel. This technique is tedious but keeps the incision as small as possible.
The Distal Release Of the Rib Involves Cartilaginous Separation
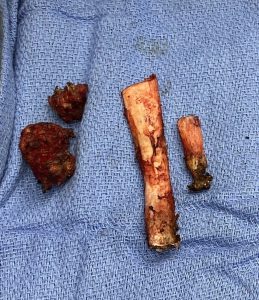
 While the proximal release of the rib in waistline narrowing surgery is bony, the distal one is cartilaginous. In rib #11 and #12 the circumferential rib dissection is carried out until the cartilaginous end segment is encountered at which point the bony rib is disarticulated from the cartilage. The cartilage segment remains behind onto which numerous musculotendinous attachments exist. There is no reason to take the small distal cartilage end…unless one is wanting to use it for a costochondral rib graft for the nose.
While the proximal release of the rib in waistline narrowing surgery is bony, the distal one is cartilaginous. In rib #11 and #12 the circumferential rib dissection is carried out until the cartilaginous end segment is encountered at which point the bony rib is disarticulated from the cartilage. The cartilage segment remains behind onto which numerous musculotendinous attachments exist. There is no reason to take the small distal cartilage end…unless one is wanting to use it for a costochondral rib graft for the nose.
The one partial exception to this approach is when rib #10 is removed. Since rib #10 is not a free floating rib its removal goes around the side until it is released from its cartilaginous continuation at the subcostal rib margin on the dorsal side of the body. This has a firm cartilaginous attachment unlike ribs #11 and #12 which are free floating segments.
Only The Bottom Three Ribs Can Be Safely Removed
Because of the location of the lung becomes closer to the ribs the higher up you go, the risk of pleural violation increases beginning at rib #10. (the lung is not close to the two bottom floating ribs) While often seen around rib #10 the pleura comes much more of an issue at rib #9…and for a cosmetic operation the risk:benefit ratio makes this not a prudent choice.
But beyond the increased risk, there is another very practical reason for leaving rib #9 alone. Which such a small incision the stretch of the tissues will only allow one rib above and below it to be reached from it. For this reason the incision is centered over rib #11. You simply can’t get to rib #9 from that far below it.
The Latissimus Dorsi Muscle Is A Major Contributor To Waistline Width
 Once past the skin incision the first major structure that is encountered is muscle, specifically the latissimus dorsi muscle. (the lats) This is one of the largest muscle in the body that stretches from the shoulder all the way down to the hip bone. Not only does this muscle go along the side of the waistline but it is also incredibly thick even down at its thinner waistline level. You have to cut through it to get to the ribs and this provides the opportunity to do some muscle remodeling as well. By taking wedges of the muscle above and below the horizontal cut at the rib #11 level this provides another waistline narrowing effect.
Once past the skin incision the first major structure that is encountered is muscle, specifically the latissimus dorsi muscle. (the lats) This is one of the largest muscle in the body that stretches from the shoulder all the way down to the hip bone. Not only does this muscle go along the side of the waistline but it is also incredibly thick even down at its thinner waistline level. You have to cut through it to get to the ribs and this provides the opportunity to do some muscle remodeling as well. By taking wedges of the muscle above and below the horizontal cut at the rib #11 level this provides another waistline narrowing effect.
Thus when you add in the flank liposuction with the muscle resection, rib removal is really a three tissue reduction approach.
Dr. Barry Eppley
Indianapolis, Indiana