

Background: Aesthetic augmentation of the midface has historically been done using a set of available standard implant shapes. Cheek and tear trough implants have their roles but are best used on top of a more normal skeletal framework for modest aesthetic enhancements. In more significant midface retrusions there is a comprehensive skeletal deficiency that can be best perceived anatomically as a ZMC rotational deficiency.
The ZMC bony component of the midface is more formally known as the zygomatico-maxillary complex. This well known union of the cheek and orbital bones forms the classic tripod, or more anatomically correct, quadrapod (four-legged) midface bone complex. It is most recognized from traumatic facial injuries and facial fracture repair. Blows or falls to the cheek area result in fracture of the ZMC’s bony legs and an inward and downward rotation of the ZMC bony complex results. This creates an external deformity of a flattened cheek and loss of undereye support. It almost always causes a traumatic negative orbital vector due to the now rescessed infraorbital rim.
For patients with significant infraorbital-malar (IOM) deficiencies with lower lid sag, scleral show and a negative orbital vector, they are somewhat like a displaced ZMC fracture. As a result the definitive approach is to augment all of the involved bony surfaces.This includes the infra- and lateral rim as well as the zygomatic body and arch. The shape of such an IOM implant would look, by definition, like a tripod.
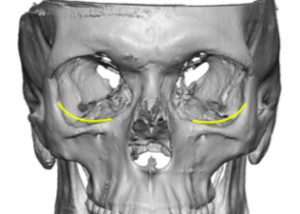
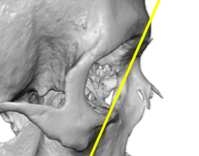
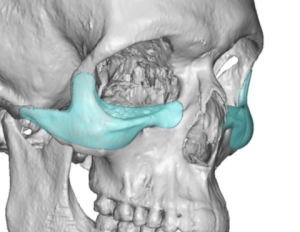
 Case Study: This male desired augmentation for his undereye hollows, flat cheeks and a negative orbital vector through an IOM implant design. His 3D CT scan showed a recessed supraorbital-infraorbital relationship, an enlarged periorbital shape due to infra-lateral rim bowing and a flat zygomatic arch shape with no bow shape to it. This is a classic Orbit0Zygomatic Complex (OZC) shape that creates his aesthetic lower eye-cheek appearance.
Case Study: This male desired augmentation for his undereye hollows, flat cheeks and a negative orbital vector through an IOM implant design. His 3D CT scan showed a recessed supraorbital-infraorbital relationship, an enlarged periorbital shape due to infra-lateral rim bowing and a flat zygomatic arch shape with no bow shape to it. This is a classic Orbit0Zygomatic Complex (OZC) shape that creates his aesthetic lower eye-cheek appearance.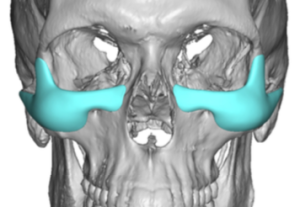
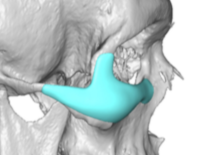
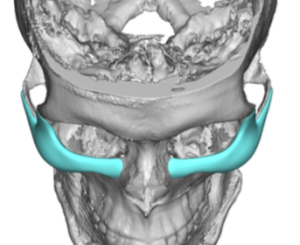
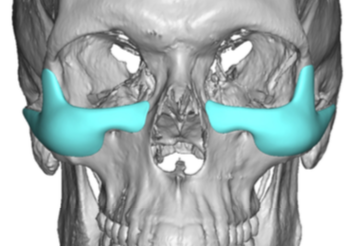
Using his 3D CT scan custom IOM implants were designed to augment the OZC bony deficiencies in a one piece implant design. The three legs of the implant included infraorbital, lateral orbital rims and zygomatic arch emanating out from a central upper zygomatic body implant design.
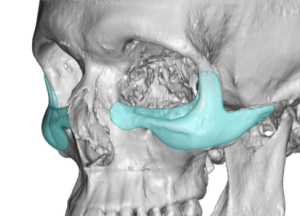 The key elements to the IOM implant design are: 1) how much to raise the height of the infraorbital rim, 2) how far up along the lateral orbital rim should the design go, 3) what is the shape of the cheek augmentation (ogee curve) and 4) how far back along the zygomatic arch should it extend.
The key elements to the IOM implant design are: 1) how much to raise the height of the infraorbital rim, 2) how far up along the lateral orbital rim should the design go, 3) what is the shape of the cheek augmentation (ogee curve) and 4) how far back along the zygomatic arch should it extend.


 During surgical placement, a lower eyelid approach is used. But not just any usual lower eyelid incision. It is a shorter length incision (only just beyond the pupil), has a very small lateral canthal extension and a full thickness skin-muscle flap is raised down to the bone. Through this very limited incision wide subperiosteal undermining is done horizontally from the medial infraorbital rim all the way out onto the end of the zygomatic arch. Vertical dissection was done up to the fronto- zygomatic suture line and down to but not past the inferior edge of the zygomatic body. The implants were then inserted in one piece through the eyelid incision by their ability to be flexed. Once into the desired position on the bone double screw fixation was applied to each side.
During surgical placement, a lower eyelid approach is used. But not just any usual lower eyelid incision. It is a shorter length incision (only just beyond the pupil), has a very small lateral canthal extension and a full thickness skin-muscle flap is raised down to the bone. Through this very limited incision wide subperiosteal undermining is done horizontally from the medial infraorbital rim all the way out onto the end of the zygomatic arch. Vertical dissection was done up to the fronto- zygomatic suture line and down to but not past the inferior edge of the zygomatic body. The implants were then inserted in one piece through the eyelid incision by their ability to be flexed. Once into the desired position on the bone double screw fixation was applied to each side.
Custom IOM implants provide the best method available for aesthetic OZC bony deformities. When you really look at the typical collection of sagging lower eyelids, undereye hollows and flat cheeks this is a reflection of a larger underlying lack of bony support. It thus makes sense that augmenting the deficient bone by onlay augmentation is the foundational maneuver. Unlike spot implant augmentations, which provide a singular hump of material in a single area, a few millimeters of implant material spread over a large bony surface area is how a custom implant design creates its effect. This more completely treats the problem and provide a platform into which other soft tissue procedures, if needed, can be performed.
Case Highlights:
1) The custom infraorbital-malar implant is the definitive approach to a OZC midfacial skeletal deficiency that is associated with a negative orbital vector.
2) The ability to create vertical height along the infraorbital rim and add horizontal projection from the infraorbital rim and out along the entire length of the zygoma in a connected fashion is the dimensional capabilities of the custom IOM implant. When it has maximal coverage it is a tripod shaped implant design.
3) The lower eyelid approach is the preferred approach for IOM implant placement.The tripod design can pose challenges for insertion through the lower eyelid incision because of its three legged shape.
Dr. Barry Eppley
Indianapolis, Indiana