


Background: The horizontal chin deficiency is the most common reason for the request for chin augmentation and standard chin implants have long been designed to address that dimensional need. But some chin deficiencies have a vertical deficiency as well which is often overlooked or whose significance is underappreciated. When standard chin implants are used in these patients an inadequate result and unhappy patient often occur.
In the combined horizontal-vertical chin deficiency the entire lower jaw is usually the culprit and orthognathic surgery may be the ideal treatment. But when an aesthetic approach is chosen the options become either a unique vertical lengthening chin implant or a bony genioplasty. What separates these two chin augmentation options is the potential behavior of the soft tissue chin pad to them. Implants can be used in these dual chin deficiencies but when the soft tissue chin pad is released it is going to need to fit over the implant at closure….and it has some limits in doing so.
 While the soft tissue chin pad definitely can be stretched when released, in the short horizontal-vertical chin deficiency the chin pad is usually smaller and tighter than normal. Thus getting it to satisfactorily pull over an implant has its limits. If the soft tissue chin pad doesn’t get completely over the implant a high riding and unnatural appearing chin shape will result. While there are no absolute numbers that apply to every patient, I have found with extensive clinical experience that when the combined horizontal and vertical increases in millimeters exceeds 12, I would be very cautious about the use of any form of an implant and a bony genioplasty is a better choice. Bony genioplasties never have a soft tissue chin pad problem because its inferior attachments never need to be released so the chin pad always follows the bone.
While the soft tissue chin pad definitely can be stretched when released, in the short horizontal-vertical chin deficiency the chin pad is usually smaller and tighter than normal. Thus getting it to satisfactorily pull over an implant has its limits. If the soft tissue chin pad doesn’t get completely over the implant a high riding and unnatural appearing chin shape will result. While there are no absolute numbers that apply to every patient, I have found with extensive clinical experience that when the combined horizontal and vertical increases in millimeters exceeds 12, I would be very cautious about the use of any form of an implant and a bony genioplasty is a better choice. Bony genioplasties never have a soft tissue chin pad problem because its inferior attachments never need to be released so the chin pad always follows the bone.
Case Study: This patient desired chin augmentation with an overall smaller lower jaw. But he was focused on chin augmentation only. Using imaging it was decided that the best aesthetic change would be a combination horizontal and vertical elongations. The deep labiomental fold should be improved by the 45 degree change in chin projection.
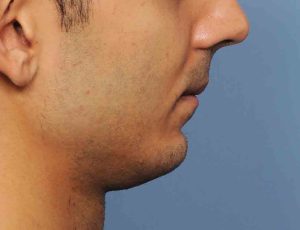


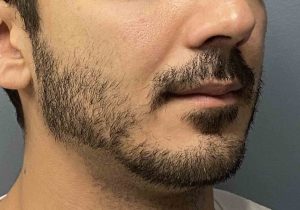
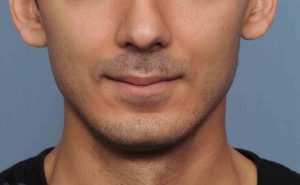
 In surgery a sliding genioplasty was done with 8mms horizontal and 5mms vertical lengthening.When seen several years later he showed a good improvement in his lower facial proportion to his upper facial thirds. Given his lower lip position his added chin projection was in alignment with it. And the labiomental fold was not deepened. (It actually appeared less deep)
In surgery a sliding genioplasty was done with 8mms horizontal and 5mms vertical lengthening.When seen several years later he showed a good improvement in his lower facial proportion to his upper facial thirds. Given his lower lip position his added chin projection was in alignment with it. And the labiomental fold was not deepened. (It actually appeared less deep)
The vertical component of a short chin is often overlooked and an implant incorrectly chosen for treatment. While a vertical lengthening chin implant has its role, significant combined horizontal and vertical projections are better served by a bony genioplasty due to its ability to carry the soft tissue chin pad along with it.
Case Highlights:
1) In the combined horizontal and vertical chin deficiency the bony genioplasty has numerous advantages over implant augmentation when the rule of 12 is exceeded.
2) The chin rule of 12 refers to the amount of combined horizontal and vertical millimeters of increase that are needed.
3) The chin rule of 12 comes from whether the detached soft tissue chin pad from a submental incisional approach can be pulled back over an implant of that dimensional size.
Dr. Barry Eppley
Indianapolis, Indiana