

Background: There are many features of the nose that affect its symmetry with the nostrils being one of them. Because they are paired structures there is always the chance of the shape and position of them can be different. The most common cause of nostril asymmetry is postoperative from rhinoplasty surgery. Due to the most commonly used open approach in rhinoplasty and changes done to the tip cartilages healing can result in nostril asymmetry which occurs along the nostril rim.This most commonly occurs at the softy tissue triangle of the nostril rim near the tip as it is unsupported by cartilage.
 But when nostril asymmetry occurs at its base this never occurs from rhinoplasty surgery unless nostril narrowing was done as part of the procedure. Nasal base asymmetry has a developmental basis and is reflected by the shape of the underlying pyriform aperture, the pair-shaped opening in the midface that extends back into the upper throat. It is surrounded by maxillary bone which has a distinct shape on its sides which extend outward from the central anterior nasal spine.
But when nostril asymmetry occurs at its base this never occurs from rhinoplasty surgery unless nostril narrowing was done as part of the procedure. Nasal base asymmetry has a developmental basis and is reflected by the shape of the underlying pyriform aperture, the pair-shaped opening in the midface that extends back into the upper throat. It is surrounded by maxillary bone which has a distinct shape on its sides which extend outward from the central anterior nasal spine.
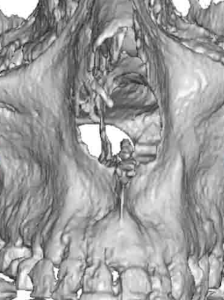 When the shape of the pyriform aperture is asymmetric it can affect the position of the overlying nostril base, where the nostril joins the face. (alar-facial groove) If the pyriform aperture is higher the nostril base above it will likely be so as well.
When the shape of the pyriform aperture is asymmetric it can affect the position of the overlying nostril base, where the nostril joins the face. (alar-facial groove) If the pyriform aperture is higher the nostril base above it will likely be so as well.
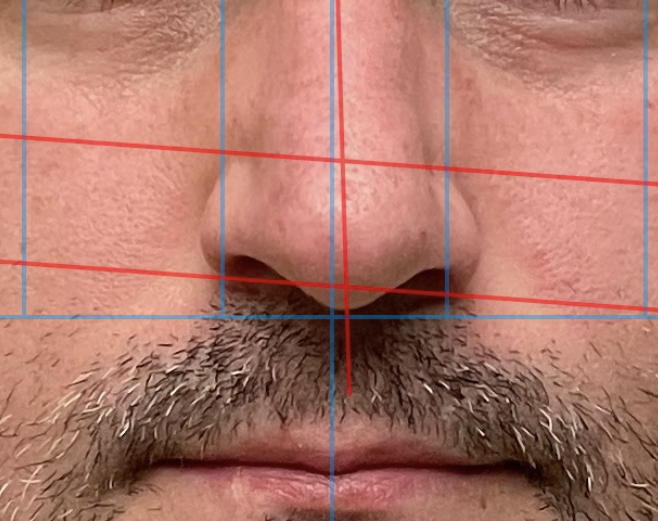
 Case Study: This male was going to undergo numerous facial procedures including a rhinoplasty. One of the features of his nose that he particularly disliked was the higher positioned right nostril. His 3D CT scan (done for his custom facial implants) showed an associated asymmetry of the pyriform aperture on that nostril side. Measured analysis of the external nostril base asymmetry showed a similar tilt to the edges of the pyriform aperture bone underneath it. He consulted with numerous surgeons for his rhinoplasty who all told him it could not be fixed and that nostril lowering could not be done.
Case Study: This male was going to undergo numerous facial procedures including a rhinoplasty. One of the features of his nose that he particularly disliked was the higher positioned right nostril. His 3D CT scan (done for his custom facial implants) showed an associated asymmetry of the pyriform aperture on that nostril side. Measured analysis of the external nostril base asymmetry showed a similar tilt to the edges of the pyriform aperture bone underneath it. He consulted with numerous surgeons for his rhinoplasty who all told him it could not be fixed and that nostril lowering could not be done.
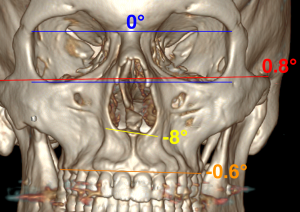
His 3D CT scan showed significant pyriform aperture bony asymmetry which had an 8 degree tilt to it at the lowest level of aperture rim.

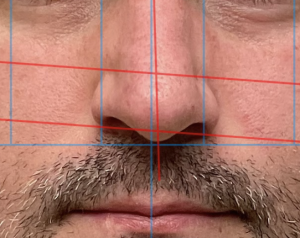
 As the final step in his rhinoplasty a curved elliptical wedge of skin measuring 3mms at the peak of its arc was excised. The nostril base was undermined and then advanced downward and closed, creating a lower alar-facial groove location.
As the final step in his rhinoplasty a curved elliptical wedge of skin measuring 3mms at the peak of its arc was excised. The nostril base was undermined and then advanced downward and closed, creating a lower alar-facial groove location.
 It is not clear as to were the belief that the nostril can not be lowered originates….as it clearly can. This specifically refers to the north-south or vertical position of the nostril. This may also be associated with lack of forward projection if the pyriform aperture has recession (increased concavity ) as well. This may necessitate augmentation of the aperture bone underneath for optimal correction./ )(which this case did not require)
It is not clear as to were the belief that the nostril can not be lowered originates….as it clearly can. This specifically refers to the north-south or vertical position of the nostril. This may also be associated with lack of forward projection if the pyriform aperture has recession (increased concavity ) as well. This may necessitate augmentation of the aperture bone underneath for optimal correction./ )(which this case did not require)
Case Highlights:
1) Congenital nostril asymmetry is often associated with an underlying asymmetry of the pyriform aperture.
2) Nostrils can be more effectively lowered than raised.
3) Nostril lowering is done by skin excision of the upper lip, changing the position of the alar-facial groove.
Dr. Barry Eppley
Indianapolis, Indiana