


Background: Having done hundreds of shoulder narrowing (clavicle reduction osteotomies) surgeries, many for transgender and a few for cis-females, there are certain anatomic observations I have made. The first is that most people’s shoulders are not not symmetric. One side is often longer and, as a result, higher than the other side. This is not necessarily related to the dominant hand but there is often preference for the left side. (which anatomic studies have also reported) But the one feature of the clavicle that is related to the dominant hand is the bone’s cross-sectional diameter. The dominant hand clavicle bone will always be thicker undoubtably due to its more frequent use and exposure to repetitive loading.
In shoulder reduction surgery some compensation for asymmetry can be done on the longer side by more bone removal. This is usually in the 3 to 5mm range which improves the asymmetry but usually not completely corrects it. With the average amount of bone removal in clavicle reduction osteotomies of 2.5cms per side there are limits as to how much additional bone can be removed. How aggressive one should be in its correction depends on the patient. Some patients are not aware of their asymmetry while others are very more sensitive to it. For those not aware efforts at correction may not be necessary at all.
The different thicknesses in the clavicles may affect how the fixation devices are applied. In the thicker dominant side, which will also be the one exposed to the higher risk of repetitive use and load bearing, double fixation plates are applied. This means that the anterior plate will be capable of having four screws placed, two on each side of the osteotomy. Conversely on the thinner side the anterior plate may be more limited in the number of screws or their bicortical placements.

 Case Study: This cis-female desired to have shoulder narrowing surgery. At 5’7” she had a bildeltoid distance of 48.5cms. Her left clavicle was longer than the right with a thicker trapezius muscle as well. The left clavicle was 5mms longer than the left at 16 mms in length with the right at 15.5cms in length. She was not aware of her shoulder asymmetry.
Case Study: This cis-female desired to have shoulder narrowing surgery. At 5’7” she had a bildeltoid distance of 48.5cms. Her left clavicle was longer than the right with a thicker trapezius muscle as well. The left clavicle was 5mms longer than the left at 16 mms in length with the right at 15.5cms in length. She was not aware of her shoulder asymmetry.
 Under general anesthesia and through supraclavicular fossa incisions 2.5cms of bone was removed from the right side and 2.75cms of bone from the left. Double plate fixation was applied.
Under general anesthesia and through supraclavicular fossa incisions 2.5cms of bone was removed from the right side and 2.75cms of bone from the left. Double plate fixation was applied.
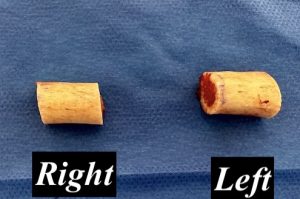
 The left clavicle bone was visible thinner than the right. As a result on the left side the anterior plate used only monocortical screws to prevent too much metal in the bone compared to the bone thickness.
The left clavicle bone was visible thinner than the right. As a result on the left side the anterior plate used only monocortical screws to prevent too much metal in the bone compared to the bone thickness.

 Her results seen on the operative table at the end of surgery showed both the reduction in shoulder width as well as improvement in the shoulder asymmetry.
Her results seen on the operative table at the end of surgery showed both the reduction in shoulder width as well as improvement in the shoulder asymmetry.
While the clavicles seem like a homogeneous bone from the outside they are rarely symmetric or similar in shape and thicknesses. Some adjustments in the amount of bone removed and how the plate and screw fixation is applied can be made for their differences which could impact healing as well as the aesthetic outcome.
Key Points:
1) Few people have symmetric clavicle lengths and shoulder shapes with the left clavicle more commonly being longer than the right.
2) Some correction of clavicle asymmetry can be done in shoulder reduction surgery by differential bone removals.
3) The dominant clavicle side is always bigger in cross-sectional diameter than the non-dominant side.
Dr. Barry Eppley
World-Renowned Plastic Surgeon