

Background: Brow bone reduction is commonly performed for female forehead feminization and the treatment of overgrown male brow bones. (masculine forehead softening) The two techniques for brow bone reduction are burring and bone flap setback, each of which has their indications. But by far the bone flap setback is the most effective form for most patients. But in some cases, by patient choice or the patient’s anatomy, a burring or shaving reduction of the anterior wall of the frontal sinus is done.
The burring method basically thins out the overlying wall of bone covering the frontal sinus and is by definition a limited form of brow bone reduction. This is done to create less horizontal projection of the brow bones. While this does accomplish reduced brow projection it often fails to fully treat all of the undesired brow bone protrusionb. At the lower end of the brow bone at the junction of the nose is an extension of the frontal sinus. This is known as the Y area of the brow bones and often undergoes under treatment in the bone flap method and always in the burring reduction method. It is a difficult area to get to by burring and the bone may not be thick enough too the burred.
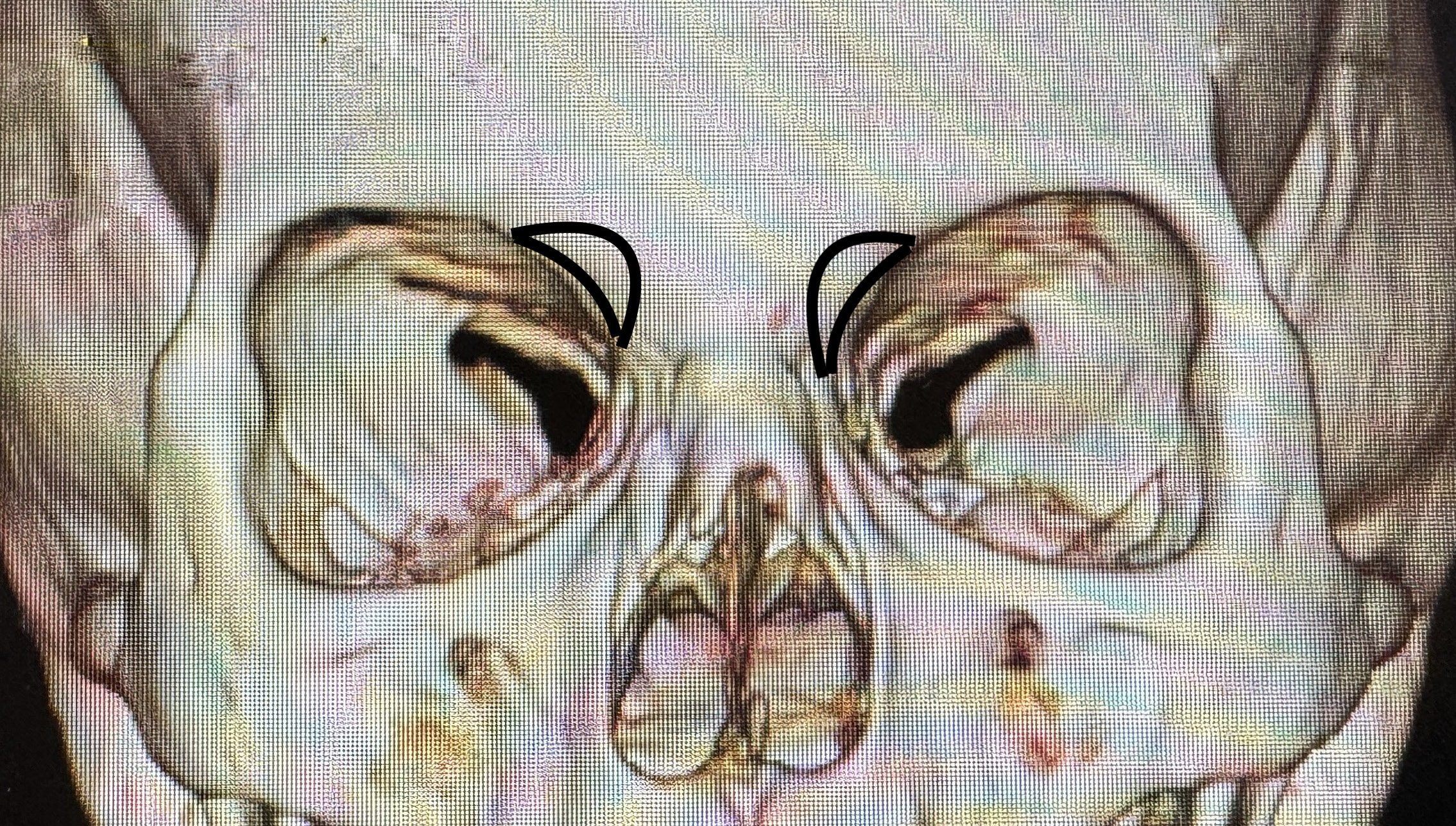
This untreated low brow bone protrusion can be seen secondarily as widening at the upper part of the nose or a divergent Y area. It would one be very appealing to try and access this area again through a reopening of the scalp incision. Can the area be accessed and reduced more readily through a more direct approach?

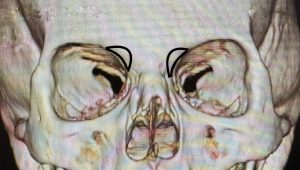
 Case Study: This female had a previous brow bone reduction done by burring through a hairline incision. The brow bone reduction result was modest but satisfactory but she was bothered by the residual widening at the low end of the medial brow bones at the frontonasal junction. (Y area) A 3D CT scan showed the bony area of widening which was caused by the bulging of the frontal sinus.
Case Study: This female had a previous brow bone reduction done by burring through a hairline incision. The brow bone reduction result was modest but satisfactory but she was bothered by the residual widening at the low end of the medial brow bones at the frontonasal junction. (Y area) A 3D CT scan showed the bony area of widening which was caused by the bulging of the frontal sinus.
 The surgical plan for reduction was small bone flaps which would be in fractured to achieve some inward reduction.
The surgical plan for reduction was small bone flaps which would be in fractured to achieve some inward reduction.

 Under general anesthesia and through 12mm skin incisions placed in the upper medial orbital area, the lower frontal sinus bulges were exposed. Using a 2mm osteotome the outliner of the bone flaps were made. Eventually they were gently infractured for a 3 to 4mm inward reduction.
Under general anesthesia and through 12mm skin incisions placed in the upper medial orbital area, the lower frontal sinus bulges were exposed. Using a 2mm osteotome the outliner of the bone flaps were made. Eventually they were gently infractured for a 3 to 4mm inward reduction.
 The incisions were closed in two layers with 6-0 plain sutures for the skin.
The incisions were closed in two layers with 6-0 plain sutures for the skin.
The Y area of the brow bones is a difficult of not impossible area to access by a burring technique. It is more easily reduced by removal of a bone flap. It is also too thin of an area to get much reduction by burring anyway. A direct bone flap reduction technique can be done with infracture that does not require plate and screw fixation if done carefully in more of a cantilever method.
Key Points:
- 1) The lower Y area of the brow bone can not be adequately addressed by a brow bone burring procedure.
2) The width at the base of the brow bones where it connects is the low anterior brow bone area mainly created by the frontal sinus.
3) Through a small upper medial orbital incision this area of the brow bone can be reduced through a small bone flap setback.
Dr. Barry Eppley
World-Renowned Plastic Surgeon