


 In placing iliac plates for pelvic bone widening its location on the bone will determine its effectiveness. The iliac crest is on the top of the wing of the ilium which flares outward at about a 45 degree angle in which it has an inner and outer lip. To optimally widen the pelvic bone the augmentation needs to be completely horizontal or as close to that direction as possible from the top of the crest. (as seen in the front view)
In placing iliac plates for pelvic bone widening its location on the bone will determine its effectiveness. The iliac crest is on the top of the wing of the ilium which flares outward at about a 45 degree angle in which it has an inner and outer lip. To optimally widen the pelvic bone the augmentation needs to be completely horizontal or as close to that direction as possible from the top of the crest. (as seen in the front view)
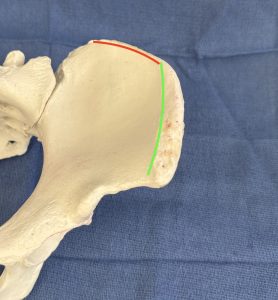 From the top view of the ilium its curved shape provides invaluable information as how to optimize implant placement for optimal width increase Based on the curve of the crest it can be divided into anterior and posterior segments. It can be seen that it is the anterior half of the crest that can create the width. The posterior section angles backward and can make no to little width contribution.
From the top view of the ilium its curved shape provides invaluable information as how to optimize implant placement for optimal width increase Based on the curve of the crest it can be divided into anterior and posterior segments. It can be seen that it is the anterior half of the crest that can create the width. The posterior section angles backward and can make no to little width contribution.
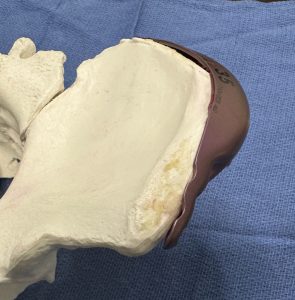
 Looking at the bony anatomy the iliac plate must be placed on the side of the iliac crest with an anterior position. It can be seen, that although the plate was designed to cover the entire iliac crest, this is unnecessary and not the optimal position. At least one hole needs to be removed posteriorly so it does not impinge onto the muscle attacghments. To get the plate as anterior as possible it may also be necessary to remove the plate and hole at its anterior end.
Looking at the bony anatomy the iliac plate must be placed on the side of the iliac crest with an anterior position. It can be seen, that although the plate was designed to cover the entire iliac crest, this is unnecessary and not the optimal position. At least one hole needs to be removed posteriorly so it does not impinge onto the muscle attacghments. To get the plate as anterior as possible it may also be necessary to remove the plate and hole at its anterior end.

 Thus iliac plate placement uses an anterior approach in the supine position. A small curved incision of 3.5cms length is made 2.5cms below and 2.5cms behind the anterior superior iliac spine. (ASIS) This not only provides good access for pocket dissection and plate placement but also is well posterior to the course of the lateral femoral cutaneous and ilioinguinal nerves. It is basically an anterior hip dip incision.
Thus iliac plate placement uses an anterior approach in the supine position. A small curved incision of 3.5cms length is made 2.5cms below and 2.5cms behind the anterior superior iliac spine. (ASIS) This not only provides good access for pocket dissection and plate placement but also is well posterior to the course of the lateral femoral cutaneous and ilioinguinal nerves. It is basically an anterior hip dip incision.

 Dissection to the crest behind the ASIS is directly down to the bone. Abdominal muscle attachments are at the inner lip and they don’t need to released. The tissues need be lifted off of the outer lip and down onto the fascia which is the tensor fascia lata anteriorly and thegluteus medius fascia the rest of the way posteriorly. The dissection needs to be as far back along the crest as the length of the plate which is in the 13cm range. Since the posterior plate holes are not used for fixation at least one of them can be removed to shorten the plate so it does not get too far back onto the posterior angled segment. Another decision is whether to keep the full three holes in the anterior section of the plate. If the most anterior hole is removed this will move the whole plate a bit more anterior, moving the maximum width projection into a more favorable position.
Dissection to the crest behind the ASIS is directly down to the bone. Abdominal muscle attachments are at the inner lip and they don’t need to released. The tissues need be lifted off of the outer lip and down onto the fascia which is the tensor fascia lata anteriorly and thegluteus medius fascia the rest of the way posteriorly. The dissection needs to be as far back along the crest as the length of the plate which is in the 13cm range. Since the posterior plate holes are not used for fixation at least one of them can be removed to shorten the plate so it does not get too far back onto the posterior angled segment. Another decision is whether to keep the full three holes in the anterior section of the plate. If the most anterior hole is removed this will move the whole plate a bit more anterior, moving the maximum width projection into a more favorable position.
 Once the plate is positioned 3.5mm screws are used in the anterior holes only. Whether two or three screws are placed depends on whether the full complement of hole remains (three) or only two. Screws must be inserted with bicortical placement. The holes are placed with a high speed drill using a 2.2mm drill. The 3.5mm screws are then hand turned into place.
Once the plate is positioned 3.5mm screws are used in the anterior holes only. Whether two or three screws are placed depends on whether the full complement of hole remains (three) or only two. Screws must be inserted with bicortical placement. The holes are placed with a high speed drill using a 2.2mm drill. The 3.5mm screws are then hand turned into place.

 Most patients will have some semblance of a hip dip preop. The iliac plate will almost always magnify the depth of the hip dip. If needed a preformed silicone hip implant is then placed right below the iliac plate and abuts right up against it. A drain is placed and the incision closed in three layers with resorbable sutures. A good layer of fascia and muscle is closed directly over the anterior plate screw holes.
Most patients will have some semblance of a hip dip preop. The iliac plate will almost always magnify the depth of the hip dip. If needed a preformed silicone hip implant is then placed right below the iliac plate and abuts right up against it. A drain is placed and the incision closed in three layers with resorbable sutures. A good layer of fascia and muscle is closed directly over the anterior plate screw holes.
The incisions are taped and an above the knee girdle is placed for compression over the hip plate-implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon