

Background: The hip area is prone to contour indentations particularly in lean or thinner patients. While some patients may want larger hips over the flat or convex hips that they have, others want to treat a specific hip contour deformity. Located between the bony iliac crest and the prominence of the greater trochanter of the femur, lack of significant subcutaneous fat between these two creates an indentation known as a hip dip. Anatomically it occurs because it has no bony support as it follows the inward concave shape of the pelvis.
Hip augmentation is a common request due to its proximity to the buttocks and injections are the primary method to do so. While synthetic fillers could be considered a first option they are less frequently done in the U.S. for various regulatory and financial reasons Fat is more commonly the injectate but when it is not available to harvest or has failed to have a sustained effect implants are the next and only option.
While a variety of body implants are available there are no standard off the shelf hip implants despite a patient need for them. Due to regulatory issues there may never be true hip implants that are marketed such. As a result surgeons have used a variety of other implants for hip augmentation which accounts for a wide variety of unpredictable results. In my experience I have always had hip implants custom made based on measurements of the desired augmented hip area. One advantages of custom implant designing is that various features can be built into the hip to either avoid potential implant complications and improve their long term results.
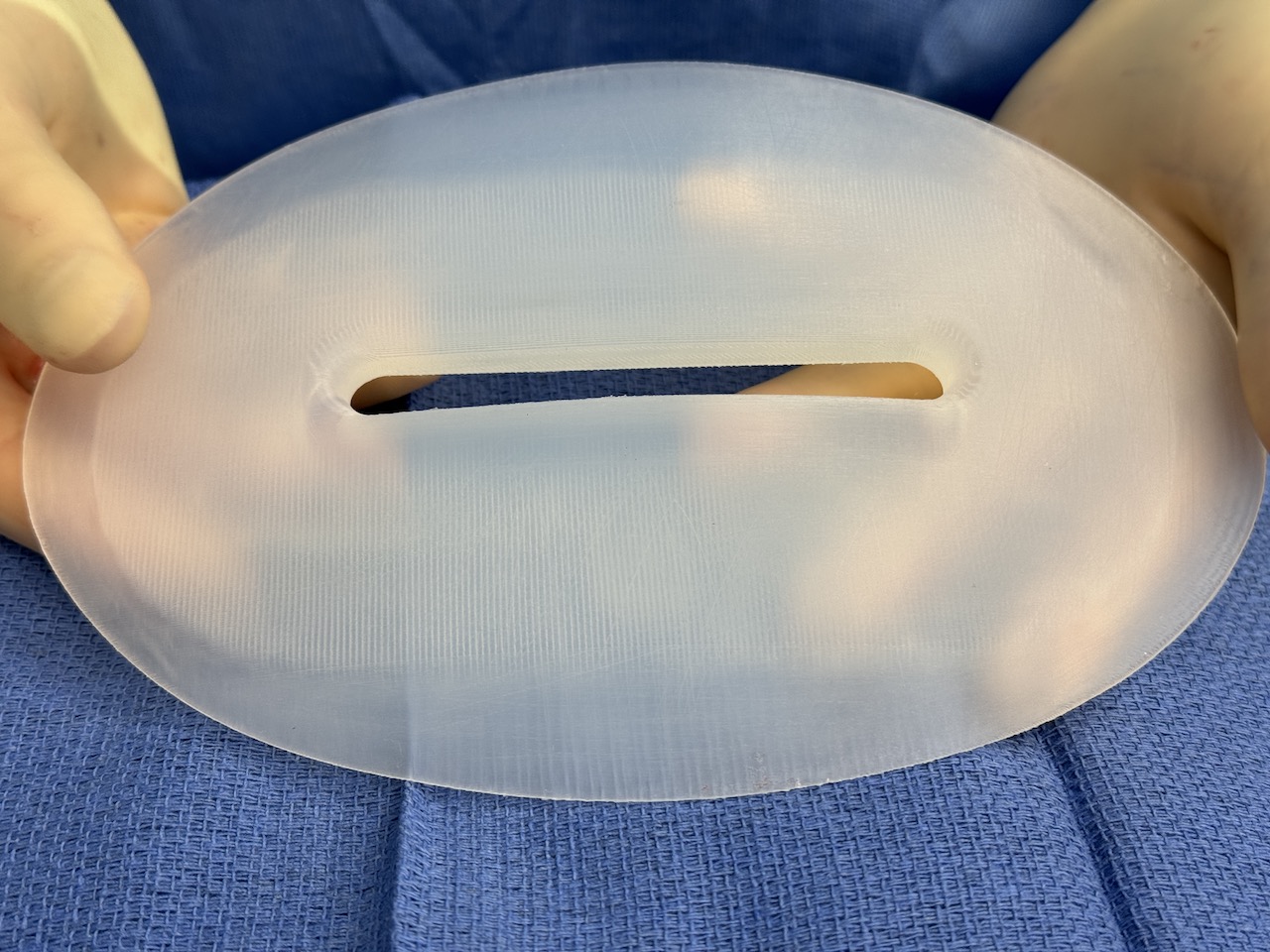
One challenging and unique aesthetic mplication with hip implants is inferior edge bending or folding. As the hip implant is vertically oriented, the bottom edge is feathered and its anatomic position is in top of the fascia, then weight of the implant can cause its lower edge to buckle creating an external bulge at the lower end of the implant. One method to counter this problem is to increase the stiffness or firmness of the implant but this often leaves the patient feeling the implants are too hard. Another strategy is to create channels in the implant so that tissue can grow through it and grab onto the implant holding its weight upright.

 Case Study: This female desired augmentation of her hip dips. She had prior fat injections to them but predictably with her lean body frame they disappeared shortly thereafter. Based on her hip dip measurements custom hip implants with a central vertical full thickness channel and ePTFE sheeting bonded to their inner surface.
Case Study: This female desired augmentation of her hip dips. She had prior fat injections to them but predictably with her lean body frame they disappeared shortly thereafter. Based on her hip dip measurements custom hip implants with a central vertical full thickness channel and ePTFE sheeting bonded to their inner surface.

 Under general anesthesia and in the side to side position, the hip implants were placed through 4.5cm skin ncisions just below the iliac crest. Dissection was through the superficial fascial layer down to the deep TFL fascia. The pockets were developed on top of the deep fascial using the external markings as to the perimeter of the pocket needed for the implant. The implants were placed over a drain and the incisions closed in multiple layers.
Under general anesthesia and in the side to side position, the hip implants were placed through 4.5cm skin ncisions just below the iliac crest. Dissection was through the superficial fascial layer down to the deep TFL fascia. The pockets were developed on top of the deep fascial using the external markings as to the perimeter of the pocket needed for the implant. The implants were placed over a drain and the incisions closed in multiple layers.

 The drains will stay in place for about a week to decrease the risk of seroma formation. The immediate and early effects of the hip implants are encouraging.
The drains will stay in place for about a week to decrease the risk of seroma formation. The immediate and early effects of the hip implants are encouraging.
It will take up to 3 months after surgery to determine how effective these implant strategies are reducing/eliminating inferior implant sag and whether the central channel will create any indentation externally.
Key Points:
1) When fat injections fail custom implants are the best approach to elimination hip dips.
2) Hip implants are prone to inferior edge folding due to lack of adhesion to the capsule for which multiple implant designs have been tried to eliminate that aesthetic problem.
3) The side to side intraoperative positioning is the most accurate method of hip implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon