

Background: There are limited options for autologous or bony jaw augmentation methods. The most well known and used is the sliding genioplasty but this is limited to the chin. Lesser known is the chin wing osteotomy, touted as a complete jaw augmentation method but it is limited by the bone cuts to the anterior 2/3s of the jawline. It can create no dimensional changes to the jaw angles and often can make the shape of them les defined and more irregular in shape.
As a result some chin wing patients need to go on to an implant-based method of jaw augmentation if they desire a more complete 3D change. The custom jawline implant is the definitive jaw augmentation method to do so. This wrap around implant can be placed over a mandible that has had a prior chin wing procedure but there will be some challenges in doing so. The elevation of the soft tissues off of the bone will be more adherent and the indwelling hardware can make passage and placement of the implant onto the bone more difficult.
But the one consideration from the prior chin wing procedure that can have the biggest concern in custom jawline implant placement is the extended intraoral vestibular incision needed to do it. Delayed healing from the original procedure may portend similar problems which if ti occurs over an implant increases the risk of infection. There is also the patient which have an unfavorable memory of the recovery from the bony procedure and may want to avoid any further intraoral surgery.
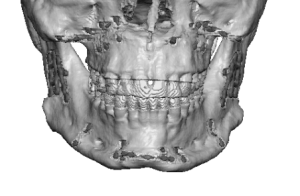
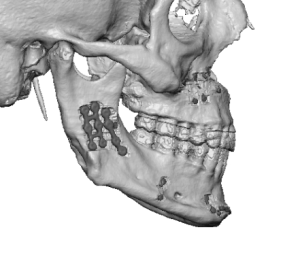 Case Study: This male desired a jaw augmentation after having had Bimax surgery with a chin wing osteotomy several years previously. His 3D CT scan show the bony changes throughout his lower jaw with a large a minute of hardware present.
Case Study: This male desired a jaw augmentation after having had Bimax surgery with a chin wing osteotomy several years previously. His 3D CT scan show the bony changes throughout his lower jaw with a large a minute of hardware present.
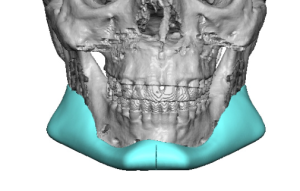
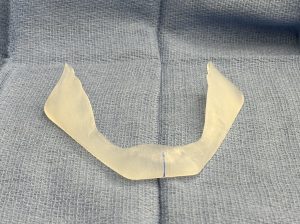
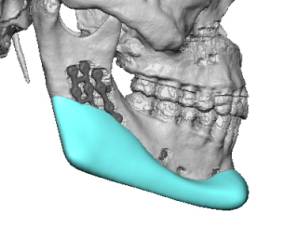 To achieve his desired lower facial change a custom jawline implant was designed of some size having a total of 19ccs of volume. The most significant reshaping change was at the deformed jaw angles.
To achieve his desired lower facial change a custom jawline implant was designed of some size having a total of 19ccs of volume. The most significant reshaping change was at the deformed jaw angles.
Per his preference he preferred not to use any intraoral incisions and wanted only an external approach.
![]() Under general anesthesia an external three incisional approach was used with an anterior submental and bilateral jaw angle skin incisions. Dissection was dissection was uncomplicated and it could be seen at the jaw angles that the intraoral approach was unlikely to do an adequate dissection around the jaw angles or get type implant into good position.
Under general anesthesia an external three incisional approach was used with an anterior submental and bilateral jaw angle skin incisions. Dissection was dissection was uncomplicated and it could be seen at the jaw angles that the intraoral approach was unlikely to do an adequate dissection around the jaw angles or get type implant into good position.

![]() The chin was initial secured in the midline with bilateral 15mm drilled screws. The jaw angles of the implant was secured with a single 16mm screw over side.
The chin was initial secured in the midline with bilateral 15mm drilled screws. The jaw angles of the implant was secured with a single 16mm screw over side.
![]()
![]() Closure of the incisions over the jaw angles showed their small size which was still adequate to get proper placement of the implant on both sides.
Closure of the incisions over the jaw angles showed their small size which was still adequate to get proper placement of the implant on both sides.
![]()
![]() He was seen over the next few weeks with very good early healing of the jaw angle incisions.
He was seen over the next few weeks with very good early healing of the jaw angle incisions.
![]()
![]() The jaw augmentation effect was clearly evident at 2 weeks after the surgery with some swelling that still needed to go down.
The jaw augmentation effect was clearly evident at 2 weeks after the surgery with some swelling that still needed to go down.
![]()
![]() The transcutaneous approach to the placement of a custom jawline implant is not new but very infrequently used. It is indicated when there has been a history of infection in prior implants that have been removed, concerns about the ability of the intraoral incisions to heal from prior surgeries or by patient preference. This incision used is a direct angle incision not a lower in the neck Risdon incision. It is right t the edge of the beard line and as a result heals very well…between than a Risdon incision in my experience and much less risk to the marginal mandibular branch of the facial nerve.
The transcutaneous approach to the placement of a custom jawline implant is not new but very infrequently used. It is indicated when there has been a history of infection in prior implants that have been removed, concerns about the ability of the intraoral incisions to heal from prior surgeries or by patient preference. This incision used is a direct angle incision not a lower in the neck Risdon incision. It is right t the edge of the beard line and as a result heals very well…between than a Risdon incision in my experience and much less risk to the marginal mandibular branch of the facial nerve.
Key Points:
1) The chin wing osteotomy can leave the jawline irregular and can not achieve a 3D dimensional augmentative change.
2) The extended intraoral incisions used for a chin wing osteotomy and the recovery from them can make patients prefer to avoid re-opening them again.
3) The transcutaneous approach for a custom jawline implant placement may be preferred by patient preference and lowers the risk of infection and implant malpositioning.
Dr. Barry Eppley
World-Renowned Plastic Surgeon