

Background: Bimaxillary or double jaw advancement surgery is a very effective procedure for obstructive sleep apnea in properly selected patients. By moving the maxillomandibular bony complex forward by a significant amount, usually 8 to 10mms, the nasal and oropharyngeal airway space is opened up for improved air flow. While functionally effective the tradeoff for such jaw movements is that what lies above the Lefort I osteotomy line will be aesthetically ‘left behind’. The infraorbital rims and zygomatic bones can often look deficient as a result creating undereye hollows and cheek flatness. This unintended effect will be even pronounced if the patient had lack of midface projection initially.
The definitive treatment for these upper midface bony deficiencies is onlay implant augmentation. There is no effective bony repositioning procedure. The complex surface anatomy of the upper midface can only be comprehensively augmented with an implant design if it is created from the patient’s 3D CT scan. When considering the implant design thought also has to be given to how the implants will be placed. (intraoral vs transpalpebral (lower eyelid) incisional approach) Each has their advantages and disadvantages.
The intraoral approach provide a scarless approach and uses an incisional scar that already exists.But its disadvantage is that getting an implant up and around the infraorbital nerve and onto the rim and out onto the cheeks can be challenging and risks an increased infection rate, permanent nerve numbness and implant malpositioning. Going through the lower eyelid lowers the risk of infection, assures better implant placement and minimizes the risk of any nerve injury. The key to the incisional approach is the implant design and how much of infraorbital rim augmentation is planned.
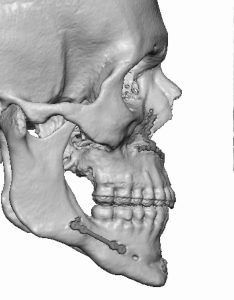
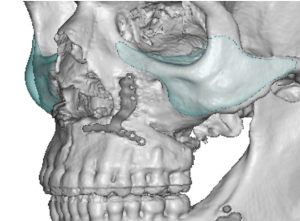
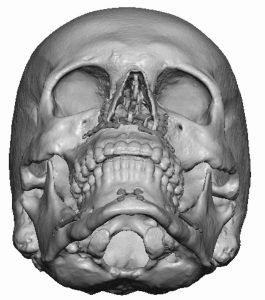 Case Study: This young male had a 14 mm bimaxillary advancement in an already lean face. The gap in the healed sagittal split was a testament to the amount of forward mandibular movement. The maxillary movement left a concave bone shape. The left cheek was appreciably asymmetric and more setback than the right side. This undoubtably existed before the bimax surgery but has become more exaggerated afterwards.
Case Study: This young male had a 14 mm bimaxillary advancement in an already lean face. The gap in the healed sagittal split was a testament to the amount of forward mandibular movement. The maxillary movement left a concave bone shape. The left cheek was appreciably asymmetric and more setback than the right side. This undoubtably existed before the bimax surgery but has become more exaggerated afterwards.
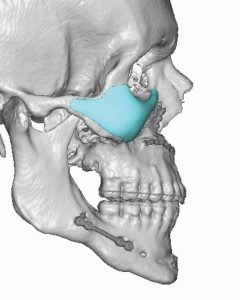
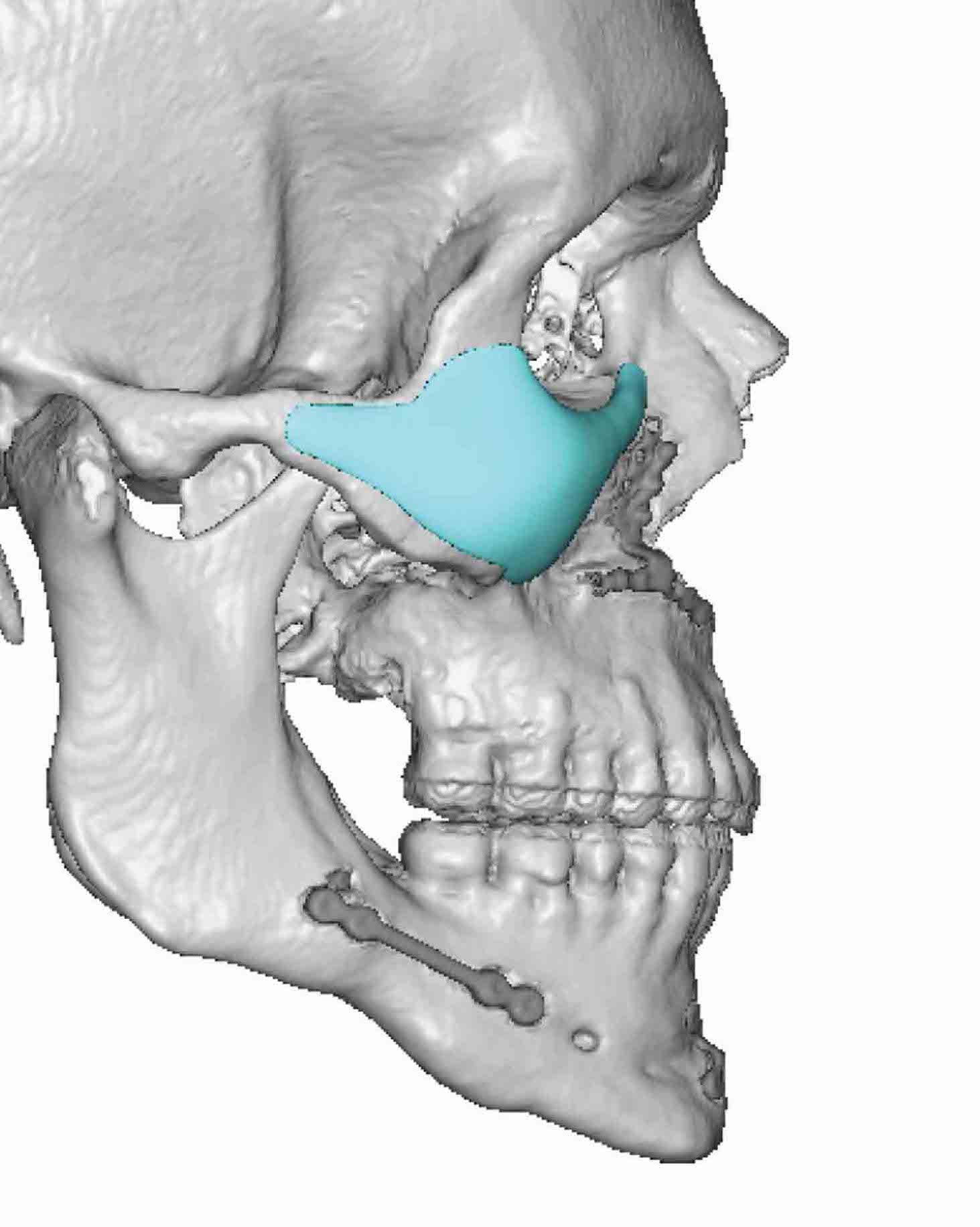
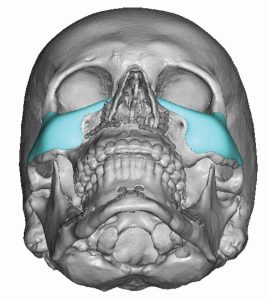 Custom infraorbital-malar (IOM) implants were designed to help with the skeletonized upper facial appearance. Malar projections of 4 and 6mms were used to help improve the cheek asymmetry resulting in implant volumes of 3ccs on the right and 4.2ccs on the left. The implant design extended across the infraorbital rims and saddled over it to provide a 3d augmentation effect.
Custom infraorbital-malar (IOM) implants were designed to help with the skeletonized upper facial appearance. Malar projections of 4 and 6mms were used to help improve the cheek asymmetry resulting in implant volumes of 3ccs on the right and 4.2ccs on the left. The implant design extended across the infraorbital rims and saddled over it to provide a 3d augmentation effect.

 Under general anesthesia and through subtotal subciliary lower eyelid incisions the custom IOM implants were placed and secured with a single microscrew per side.
Under general anesthesia and through subtotal subciliary lower eyelid incisions the custom IOM implants were placed and secured with a single microscrew per side.

 When seen four months later the implants provided a good volumetric effect without looking overdone or disportionatelyout of place.They still kept his lean face look but he no longer had a gaunt appearance or a too skeletonized upper midface appearance.
When seen four months later the implants provided a good volumetric effect without looking overdone or disportionatelyout of place.They still kept his lean face look but he no longer had a gaunt appearance or a too skeletonized upper midface appearance.
 Complete skeletal restoration of the deficienct upper midface after a significant LeFort I osteotomy would technically be augmentation of the upper maxilla, infraorbital rim and zygomatic body. Such an implant design would be hard to place adequately from either an intraoral or a lower eyelid approach. (unless a two piece midface implant design is made and is placed in two pieces using both approaches) But the most visible part of the deficiency is around the more convex shaped bone around the eye and cheeks. Even though the custom IOM implants only provide an incomplete restoration they are usually aesthetically adequate in most cases.
Complete skeletal restoration of the deficienct upper midface after a significant LeFort I osteotomy would technically be augmentation of the upper maxilla, infraorbital rim and zygomatic body. Such an implant design would be hard to place adequately from either an intraoral or a lower eyelid approach. (unless a two piece midface implant design is made and is placed in two pieces using both approaches) But the most visible part of the deficiency is around the more convex shaped bone around the eye and cheeks. Even though the custom IOM implants only provide an incomplete restoration they are usually aesthetically adequate in most cases.
Key Points:
1) Major bimaxillary advancement surgery will leave the upper midface behind creating undereye hollows and cheek flatness.
2) Custom infraorbital-malar implants provide a partial aesthetic correction of the upper midface deficiency.
3) In designing custom infraorbital-malar implants for largely increased anterior projection the infraorbital component must saddle the rim to provide adequate forward projection.
Dr. Barry Eppley
World-Renowned Plastic Surgeon