

Background: The tip of the nose is essentially a collection of free-floating cartilages that is suspended by ligaments to the rigidly fixed upper lateral cartilages and septum. This is why the tip of the nose is freely mobile which helps protect it against trauma. Some have appropriately described the nasal tip like a spring of which mechanically is a useful concept when looking at reductive or augmentative of nasal tip changes.
Because of its free mobility the nasal tip can readily be rotated upward and/or shortened. These are the most common nasal tip changes, along with making it less wide, and their effectiveness has long been established. However the reverse, tip lengthening and/or derotation is not as easily accomplished. Such changes require additional structural support to achieve to provide the outward and downward push of the end of the nasal tip. Such structural support comes from cartilage grafting.
When lengthening the tip of the nose by cartlidge grafting there are two locations to provide the outward changes. For minor changes onlay grafting can be done to the infra tip area to build out the support between the skin and caudal end of the cartilages. For greater changes the end of the septum can be extended by placing a graft between it and the cephalic end of the medial foot plates of the lower alar cartilages. In some cases, particularly in thick nasal skin, it may be necessary to do both types of cartlilage tip grafting.
Case Study: This middle aged male desired changes to his nasal tip. He always felt that his nose was under developed with a tip that was too short, upturned, and broad. He had never had any prior nasal surgery. His nasal skin was moderately thick.



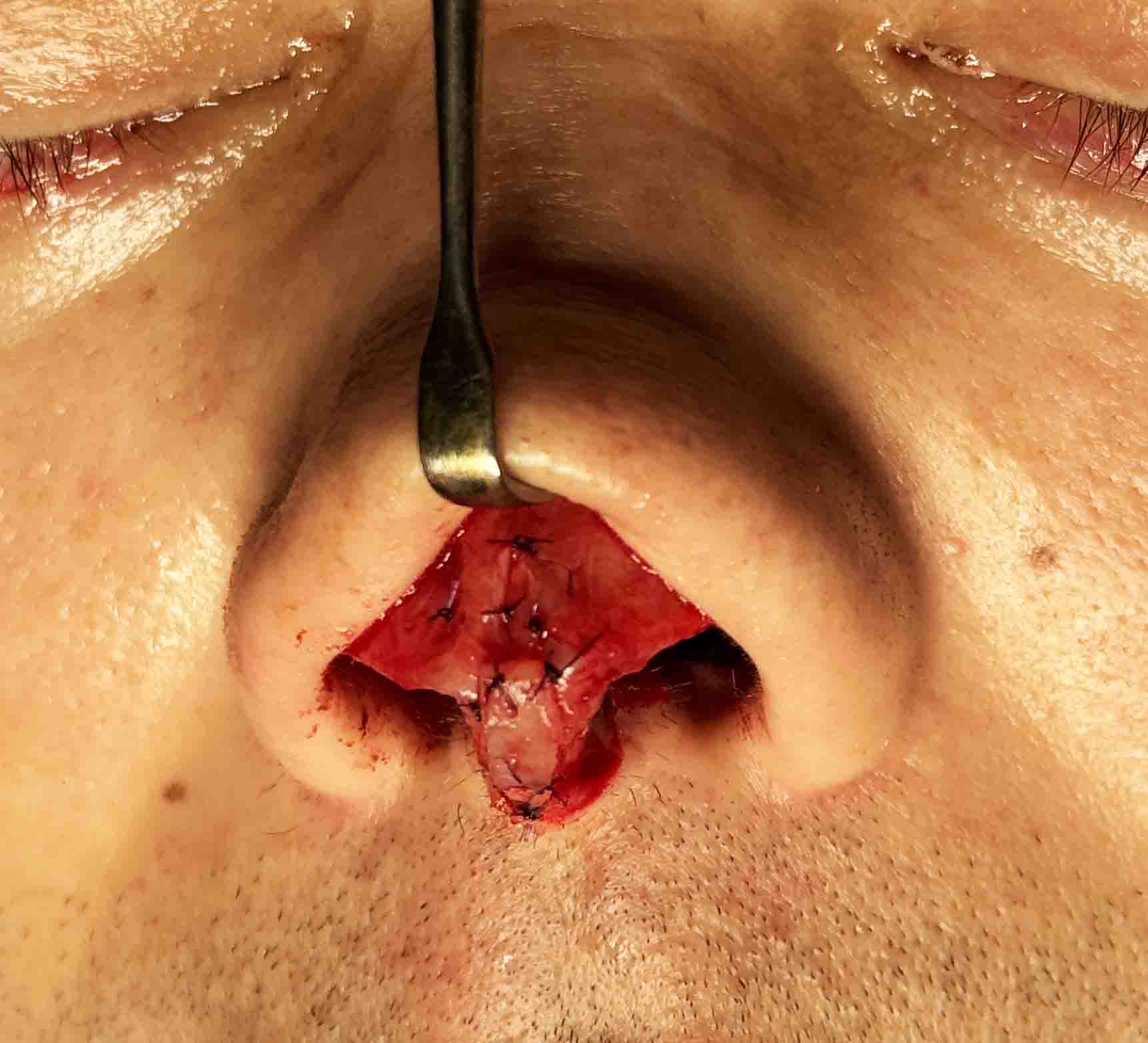
 Under general anesthesia and through and open rhinoplasty a large septal cartilage graft was initially harvested. A 1 cm septal extension graft was placed followed by infratip onlay grafting of multiple layers. The nasal tip cartilages is were also narrowed by transdomal sutures.
Under general anesthesia and through and open rhinoplasty a large septal cartilage graft was initially harvested. A 1 cm septal extension graft was placed followed by infratip onlay grafting of multiple layers. The nasal tip cartilages is were also narrowed by transdomal sutures.

 When seen three months later the increased tip length with less rotation was seen. He’s still had some moderate fullness in the nasal tip and steroid injections were placed to help reduce it.
When seen three months later the increased tip length with less rotation was seen. He’s still had some moderate fullness in the nasal tip and steroid injections were placed to help reduce it.
 The healing of the open rhinoplasty columellar scar was essentially undetectable at this point in the recovery.
The healing of the open rhinoplasty columellar scar was essentially undetectable at this point in the recovery.
Lengthening the nasal tip is much harder than shortening it and, as can be seen in this patient even with maximal cartilage grafting, the changes are visible but not necessarily dramatic. Fortunately for this patient this was exactly the type of change that he desired. Ultimately what controls the ability to lengthen the nasal tip is a combination of the tightness of the nasal skin as well as how much cartilage grafts are applied. Lengthening the tip of the nose will also help with its narrowing, along with the suture placements, due to the stretch on the nasal tissues.
Key Points:
1) The tip of the nose can be lengthened or shortened of which the former is more challenging to achieve than the latter.
2) The tip of the nose can also be lift or brought down of which the latter is more difficult to do than the former.
3) Tip lengthening and derotation requires maximal cartilage grafting to achieve a visible change.
Dr. Barry Eppley
World-Renowned Plastic Surgeon