

The most common potential adverse affect relating to facial implants is the concern about bone erosion. While this is certainly not the most common complication from facial implants it is certainly one that is widely spoken about albeit biologically incorrect. The term erosion goes back over 50 years from looking at some chin implants in lateral cephalometric x-rays. It could be seen that in some patients that the implant has settled into the bone. This was particularly evident in implants that were positioned high on the chin bone where the outer cortex is thinner. (and under more pressure from the origin of the mentalis muscle.) In very rare cases the tooth roots may be at risk.
As a result of these historic x-ray findings facial implants, particularly chin implants, have become associated with causing long term bone loss. But this interpretation of what happens around lower facial implants fails to appreciate the actual biology of how the body responds to the interposition of an implant into its tissue planes. Since a plain x ray served as the basis for the erosion supposition more contemporary 3D CT scan imaging shows a different and more complete understanding of the biologic response to the placement of an implant on the mandible.
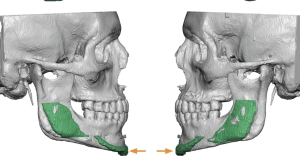
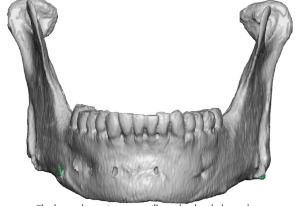 Having looked at thousands of 3D CT scans with facial implants on them and then digitally removing them for new custom implant designs, what happens around and under an implant can more clearly be appreciated. What is seen are variables patterns of the implant on the bone. (imprinting) Some implant imprints are very faint almost non-discernible while others are more evident. These implant patterns occur regardless of the implant material used, implant shape or size of the implant. They are most distinct on the mandible and are less significant higher up on the face. (faint to no imprinting)
Having looked at thousands of 3D CT scans with facial implants on them and then digitally removing them for new custom implant designs, what happens around and under an implant can more clearly be appreciated. What is seen are variables patterns of the implant on the bone. (imprinting) Some implant imprints are very faint almost non-discernible while others are more evident. These implant patterns occur regardless of the implant material used, implant shape or size of the implant. They are most distinct on the mandible and are less significant higher up on the face. (faint to no imprinting)

 But what is also seen are variables amount of bony over growths around the edges of the implant. In both chin and jaw angle implants most of the bony overgrowths come from the top side of the implants. Only when the implant is positioned too high on the bone are bony overgrowths seen from the bottom side of the implant. Such bony overgrowths are almost never seen in the midface and forehead.
But what is also seen are variables amount of bony over growths around the edges of the implant. In both chin and jaw angle implants most of the bony overgrowths come from the top side of the implants. Only when the implant is positioned too high on the bone are bony overgrowths seen from the bottom side of the implant. Such bony overgrowths are almost never seen in the midface and forehead.
What does these 3D CT scan findings tell us about the biology of facial implants? First and foremost it is clear that an inflammatory reaction to them is not what is occurring. The clear and sharply defined imprint borders of the implant make that evident. If it was an inflammatory reaction (erosion) the pattern of the implant on the bone would be irregular and indistinct and have an almost ‘moth-eaten’ appearance. Secondly an inflammatory reaction would not result in any evidence of bony overgrowths. Inflammatory cells are destructive not regenerative. Bony overgrowths are a sign of a healing response, trying to heal over the implant.
The key concept to grasp in any form of aesthetic augmentation, and craniofacial augmentation in particular because the bony response can be more clearly seen, is that of the violation of anatomic boundaries. The tissues at any implantation have formed to support what has developed around them. When you introduce an implant, which exerts its augmentation effect by pressure and can not physically change its shape, the tissues around it must adapt to the pressure that has now been exerted onto them. A natural pressure relief results which is seen by some implant settling into the bone which occurs in varying degrees. Once this pressure relief has occurred it stops resulting in a response to the implant that is not progressive. (self-limiting)
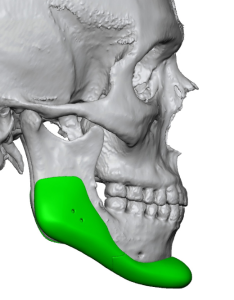
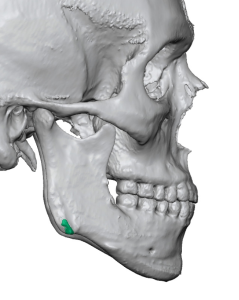 This violation of biologic boundaries has been known for some time in craniofacial surgery with the use of onlay bone grafts. Such grafts are well known to partially resorb and change their shape as they heal. As an organic material that can respond to the pressure of the tissues around them by changing their form…a response that an inorganic implant material can not do. As a result the tissues around an implant must adapt to the pressure with a relief creating a limited amount of passive bone resorption (imprinting) with a reparative response with attempts at healing bone over the implant. Interestingly as the implant becomes over a larger surface area, such as a custom jawline implant, the imprinting reaction seems to be less distinct. Perhaps this is due to the distribution of the implant pressure over a large surface area.
This violation of biologic boundaries has been known for some time in craniofacial surgery with the use of onlay bone grafts. Such grafts are well known to partially resorb and change their shape as they heal. As an organic material that can respond to the pressure of the tissues around them by changing their form…a response that an inorganic implant material can not do. As a result the tissues around an implant must adapt to the pressure with a relief creating a limited amount of passive bone resorption (imprinting) with a reparative response with attempts at healing bone over the implant. Interestingly as the implant becomes over a larger surface area, such as a custom jawline implant, the imprinting reaction seems to be less distinct. Perhaps this is due to the distribution of the implant pressure over a large surface area.
Dr. Barry Eppley
World-Renowned Plastic Surgeon