

Background: The clavicle is the only horizontally oriented bone in the body whose primary function is to keep the shoulder at a distance from the sternum and ribcage. But do doing the arm can have an adequate range of motion. It is a load-bearing bone in which its size (defined as its diameter) will be influenced by the body frame it is on and the force loading to which it has been exposed based on the person’s lifestyle. As a result there are several features of the clavicle bone that are predictable. Male clavicles are going to be bigger on average than most females. The right clavicle, if the person is right handed, will be bigger than the left side. Similarly the right clavicle due to increased use, provided they are right handed, will have more curvature at its two ends than the opposite side.
While these may seem to be just interesting bone observations but when it comes to clavicle reduction surgery they are very relevant. The size or the diameter of the bone affects how much plate and screw fixation is applied when it gets put back together. In a normal or bigger size clavicle I typically apply double plate fixation. (a larger plate on top and a smaller plate on the front side of the bone) This is because the bone size will permit it as well as a concern as to the load to which the fixation will be asked to endure as it heals. But when the clavicle bone is small (the size of my little finger) the application of double plate and screws places a lot of metal on and around the osteotomy site that could jeopardize its ability to heal. (risk of non-union) Because of this concern I will only use the superior plate to avoid this potential risk.
In most patients that present for shoulder narrowing surgery you can usually predict what the size of the clavicle bones will be. The more height and weight they have one can expect that the bone will be bigger. And this is almost always true…but not always.
Case Study: This female presented shoulder narrowing surgery. She was 5’ 10” talk and weighted 210lbs. Her bideltoid distance was 51cms with a clavicle length of 17cms. All indicators are that these would be good sized clavicle bones.
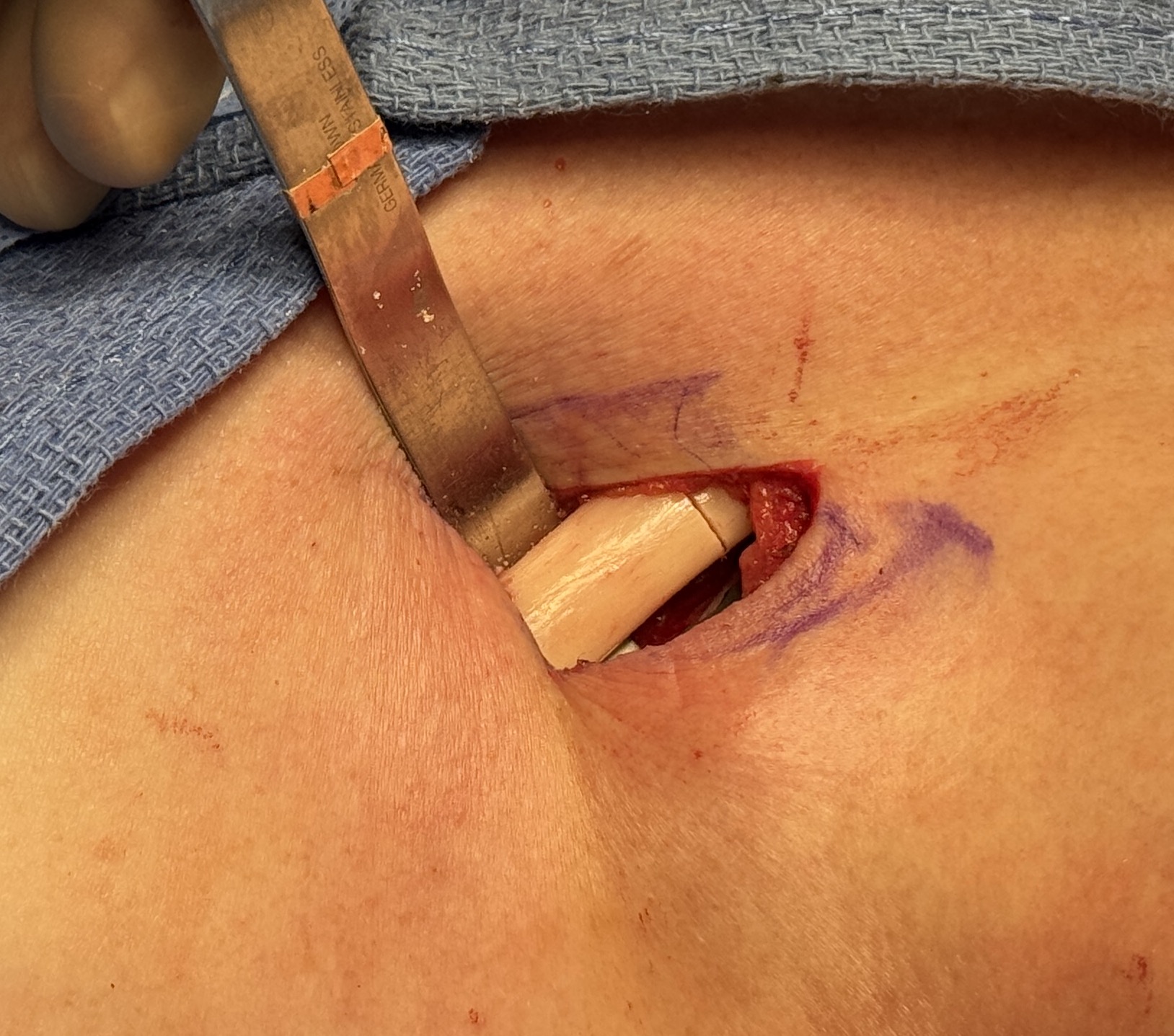
 Under general anesthesia and through 3.5cm length supraclavicular incisions the clavicle bone were exposed and were found to be remarkably small…certainly smaller than expected. The left side was actually bigger than the right even though it was small as well. They both had a round shape without a typical flat top to its superior surface. The diameters of the bone were 15mms or less.
Under general anesthesia and through 3.5cm length supraclavicular incisions the clavicle bone were exposed and were found to be remarkably small…certainly smaller than expected. The left side was actually bigger than the right even though it was small as well. They both had a round shape without a typical flat top to its superior surface. The diameters of the bone were 15mms or less.

 The bone was resected from the straight portion of the bone underneath the incision and the superior plate was applied. There was just enough room to place a small anterior plate and I almost did not do it because of how thin the bone was. But given the size of the patient I felt more fixation was better than less. In looking at the bone through the incision all you could see are the plates. But to hedge against the risk of too much metal to bone the anterior plate, which acts as a stabilizing plate, had only one screw per side of the two bone ends.
The bone was resected from the straight portion of the bone underneath the incision and the superior plate was applied. There was just enough room to place a small anterior plate and I almost did not do it because of how thin the bone was. But given the size of the patient I felt more fixation was better than less. In looking at the bone through the incision all you could see are the plates. But to hedge against the risk of too much metal to bone the anterior plate, which acts as a stabilizing plate, had only one screw per side of the two bone ends.



 Immediately after surgery she had good reduction of her shoulder width and shape.
Immediately after surgery she had good reduction of her shoulder width and shape.
 Her postoperative x-ray showed good alignment of both clavicle reduction sites.
Her postoperative x-ray showed good alignment of both clavicle reduction sites.
Key Points
1) Broad shoulders can be successfully reduced by a typical amount of clavicle bone removal.
2) The larger the body frame is in height and weight one can usually expect a similarly large clavicle bone in diameter.
3) When the clavicle bone is small in diameter the decision in clavicle reduction osteotomies is whether one or two plates should be used.
Dr. Barry Eppley
World-Renowned Plastic Surgeon