

The clavicle reduction osteotomies used in aesthetic shoulder narrowing surgery is conceptually straightforward. Remove a specific length of bone, pull the remaining two ends of the bone back together and put a plate and screws to hold it together so it heals. This would be fairly easy if one is working on a skeletal model but doing it through a limited skin incision is a different matter.
One of the hardest parts of the surgery is to bring the two ends of the clavicle together with a good close end to end approximation. That may seem easy but lifting up the shoulder, bringing the outer end of the bone in and putting its small end up against the other small end…and then hold it there long enough to put on the plate and screw fixation is physically challenging. It actually takes three people to do it successfully.

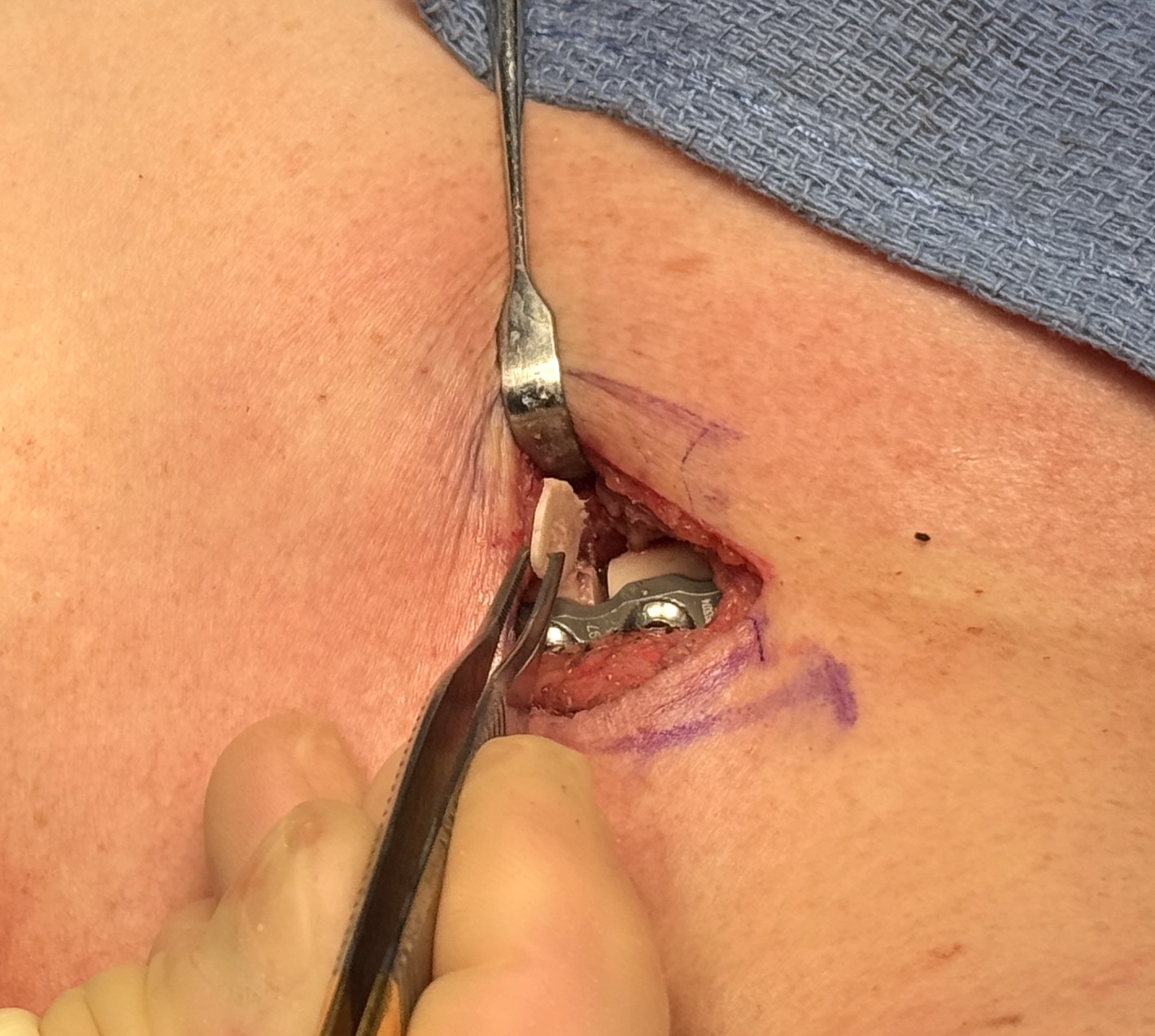
 But despite the best efforts to push the two bone ends tightly together when the plate and screws are applied there can be some slight gap between the two ends. It may be that it would go on to heal despite this small gap (1 to 1.5mms) but I don’t like seeing it and there is a ready bone graft source available. One of the removed bone segments can be used and a reciprocating saw can cut off a very thin wedge of bone from it. This bone wedge can be then placed into the gap for a perfect fit between the two ends.
But despite the best efforts to push the two bone ends tightly together when the plate and screws are applied there can be some slight gap between the two ends. It may be that it would go on to heal despite this small gap (1 to 1.5mms) but I don’t like seeing it and there is a ready bone graft source available. One of the removed bone segments can be used and a reciprocating saw can cut off a very thin wedge of bone from it. This bone wedge can be then placed into the gap for a perfect fit between the two ends.
 Since forceps to put the two bone ends together under compression is not possible through the small incision used manual end to end approximation has to be used. Despite best efforts small gaps between the two ends can sometimes occur and can easily be bone grafted. Such wedge bone grafts are so small/thin they can not be seen in an x-ray.
Since forceps to put the two bone ends together under compression is not possible through the small incision used manual end to end approximation has to be used. Despite best efforts small gaps between the two ends can sometimes occur and can easily be bone grafted. Such wedge bone grafts are so small/thin they can not be seen in an x-ray.
Dr. Barry Eppley
World-Renowned Plastic Surgeon