

Background: Wide or excessive convex shaped sides of the head are associated with both aesthetic and occasional functional symptoms. Aesthetically the side of the head is generally desired to be straight and not convex or bowed out. When it is excessively wide both the shape of the bone and the thickness of the muscle can contribute to this wide shape but their contributions to the head width are not necessarily equal.
Contrary to common perception the contribution of the temporal bone to head width is due to an increased convexity of the bone and not increased bone thickness. The temporal bone is naturally thin often being only 5mms or less thick. It is an exaggeration of its natural convexity that creates a bowed out appearance in which the bone may even be thinner than normal as a result.
The temporal muscle, however, can be quite different. Its thickness can vary but is not directly correlated to the thickness or increased convexity of the underlying bone. To the contrary the muscle over the bony convexity can be quite thick even though it is always thinner than the anterior part of the muscle which lies in the concave temporal fossa. When thick enough it is this muscle which is removed to help make the sides of the head straighter. Its removal causes no functional issues as the remaining thick fossa muscle is more than adequate for normal jaw function.
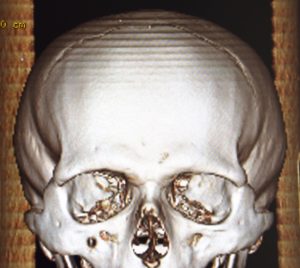
 Case Study: This male had a very wide head shape with increased bitemporal head width. His 3D CT scan showed that the shape of the temporal bone was convex and wide. Coronal sections of the CT showed the bowed out shape of the temporal bone but also that it was very thin. The temporal muscle over the convex part of the temporal bone was much thicker than the bone itself. This made him a good candidate for a temporal muscle reduction surgery.
Case Study: This male had a very wide head shape with increased bitemporal head width. His 3D CT scan showed that the shape of the temporal bone was convex and wide. Coronal sections of the CT showed the bowed out shape of the temporal bone but also that it was very thin. The temporal muscle over the convex part of the temporal bone was much thicker than the bone itself. This made him a good candidate for a temporal muscle reduction surgery.

 Under general anesthesia and through a postauricular incision the deep temporal fascia was exposed. The fascia was opened, leaving a cuff of muscle and fascia inferiorly, and a cut made down through the muscle to the bone.
Under general anesthesia and through a postauricular incision the deep temporal fascia was exposed. The fascia was opened, leaving a cuff of muscle and fascia inferiorly, and a cut made down through the muscle to the bone.
 The muscle thickness at the level just above the ear measured 12mms on each side.
The muscle thickness at the level just above the ear measured 12mms on each side.
 The muscle was released widely from the underlying bone and the overlying fascia by elevators. Using electrocautery a full thickness muscle cut was done int an oblique direction from the ear up to the forehead. The cut line was at the end of the convex part of the bone as it started into the concave part of the temporal fossa. The entire muscle behind this cut line was then removed.
The muscle was released widely from the underlying bone and the overlying fascia by elevators. Using electrocautery a full thickness muscle cut was done int an oblique direction from the ear up to the forehead. The cut line was at the end of the convex part of the bone as it started into the concave part of the temporal fossa. The entire muscle behind this cut line was then removed.
The temporal fascia was put back together over a drain which acts to smooth out the posterior cut edge of the remaining muscle. The postauricular skin incision was closed with resorbable sutures and a circumferential head wrap applied.

 When seen the next day for drain removal and head wrap removal the reductive change in the shape of the sides of his head could be seen the back view.
When seen the next day for drain removal and head wrap removal the reductive change in the shape of the sides of his head could be seen the back view.

 Similarly the reductive changes could be seen in the front view as well. There is some swelling in the remaining anterior temporal muscle, which will actually get worse in the following days, but the convex shape above the ears is now straight.
Similarly the reductive changes could be seen in the front view as well. There is some swelling in the remaining anterior temporal muscle, which will actually get worse in the following days, but the convex shape above the ears is now straight.
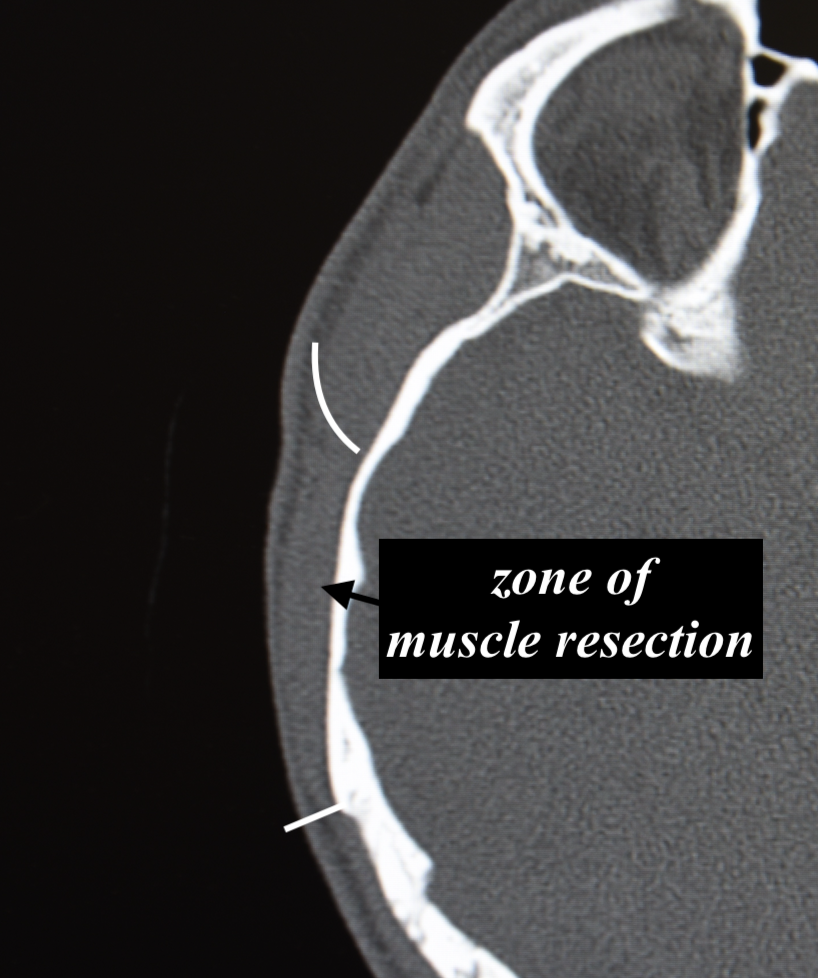
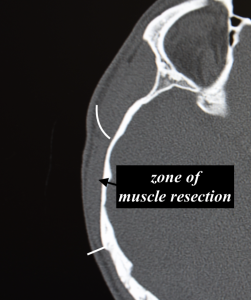 A CT scan can confirm whether temporal muscle removal would be beneficial in the wide head patient. The ratio of the muscle to the bone can be evaluated and when the muscle is thicker than the bone this is an absolute indication that it will be effective. The scan can also help appreciate where the muscle is removed which is over the convex part of the temporal bone. The muscle thickens considerably as it ascends into the deeper concave temporal fossa where it is inaccessible for effective removal.
A CT scan can confirm whether temporal muscle removal would be beneficial in the wide head patient. The ratio of the muscle to the bone can be evaluated and when the muscle is thicker than the bone this is an absolute indication that it will be effective. The scan can also help appreciate where the muscle is removed which is over the convex part of the temporal bone. The muscle thickens considerably as it ascends into the deeper concave temporal fossa where it is inaccessible for effective removal.
Key Points
1) The wide convex head shape is associated with a bony component but the muscle thickness can be making a major contribution to the side of the head width.
2) A CT scan is helpful to determine the bone vs muscle contribution to the head width and whether temporal muscle reduction would be beneficial.
3) Temporal muscle reduction involves removal of all the muscle over the convex portion of the temporal bone up into the beginning of the edge into the concave portion of the temporal bone.
Dr. Barry Eppley
World-Renowned Plastic Surgeon