

Background: Aesthetic contouring of the cheeks could involve augmentation or reduction. In either case potential treatment areas include the bone or the soft tissue. Augmentation is the most conceptually understood because that involves either an implant to augment the bone or fat injections to add volume to the soft tissues. Conversely cheek reduction means reducing the width of the cheekbones by bone removal/osteotomies or removing soft tissue volume.
The objective of soft tissue cheek reductions is to create a less full or more ideally concave appearance between the bony cheeks and jawline. The most commonly performed procedure to do is the buccal lipectomy… mainly because it is the only one that most surgeons know and the location of the buccal fad is straightforward to find. But in some cases a buccal lipectomy may not be as effective as one would like. This can occur due to either a misdiagnosis of the primary fat location or an under appreciation of the different fatty compartments of the cheeks.
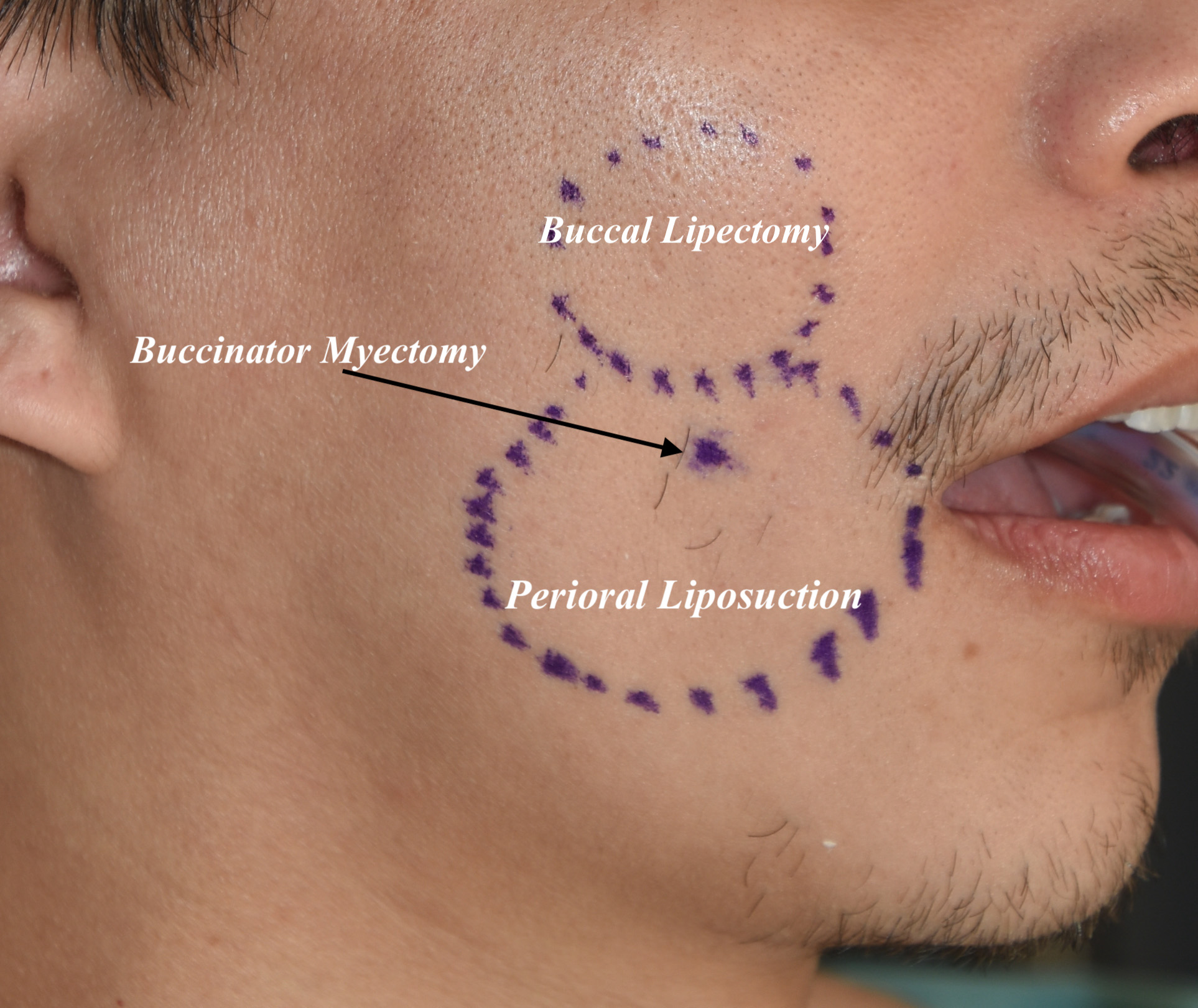
 The soft tissues of the cheek has more potential for fatty reductions than just that of the buccal fat pad. When considering soft tissue cheek reductions I think of the entire area between the cheekbones and the jawline which is not supported by bone. The soft tissues are suspended between these two bony lines and be thought of as a trampoline. Within the trampoline area lies the buccal fat superiorly and the perioral subcutaneous fat layer inferiorly which is divided between an equator line from the mouth corner up to the tragus of the ear. While the effects of a buccal lipectomy lies north of this line it is liposuction of the subcutaneous fat of the perioral area below this line that can help with an effective reduction.
The soft tissues of the cheek has more potential for fatty reductions than just that of the buccal fat pad. When considering soft tissue cheek reductions I think of the entire area between the cheekbones and the jawline which is not supported by bone. The soft tissues are suspended between these two bony lines and be thought of as a trampoline. Within the trampoline area lies the buccal fat superiorly and the perioral subcutaneous fat layer inferiorly which is divided between an equator line from the mouth corner up to the tragus of the ear. While the effects of a buccal lipectomy lies north of this line it is liposuction of the subcutaneous fat of the perioral area below this line that can help with an effective reduction.
To accompany either or both areas of cheek fat reduction is a third procedure which is a modification of the cheek dimple procedure. Making cheek dimples is about creating a discreet indentation in one small area by muscle removal and then pulling the skin externally and mucosa internally together through a suture. But this concept can be expanded to a more broader effect though a wider based open procedure known as a buccinator myectomy.
Case Study: This male desired to have a thinner soft tissue cheek trampoline area. He was already at a good lean weight so weight loss was not an option. He was happy with his cheeks, chin and jawline.
 Under general anesthesia a three procedure approach was taken to reduction of his soft tissue cheek area including buccal lipectomies, perioral liposuction and an internal buccinator myectomy.
Under general anesthesia a three procedure approach was taken to reduction of his soft tissue cheek area including buccal lipectomies, perioral liposuction and an internal buccinator myectomy.
 Through bilateral intraoral high maxillary vestibular incisions buccal lipectomies were initially performed. This was followed by small cannula liposuction of the perioral area through nick incisions just inside the mouth corners. Lastly buccinator myectomies were performed nu a horizontal excision of mucosa and buccinator muscle below the parotid duct at the level of the occlusal plane.
Through bilateral intraoral high maxillary vestibular incisions buccal lipectomies were initially performed. This was followed by small cannula liposuction of the perioral area through nick incisions just inside the mouth corners. Lastly buccinator myectomies were performed nu a horizontal excision of mucosa and buccinator muscle below the parotid duct at the level of the occlusal plane.

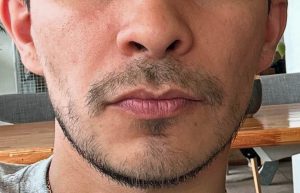 When see four years later the long term results of the reduction in the soft tissue cheek area could be appreciated.,
When see four years later the long term results of the reduction in the soft tissue cheek area could be appreciated.,
It is commonly perceived that the buccal lipectomy is the only soft tissues cheek reduction procedure. As a result it is used commonly by most surgeons for any patient request for soft tissue cheek reduction. Because of anatomic misunderstandings of its exact facial effects patients can have an unsatisfactory aesthetic improvement as seen by an inadequate reduction. This very typically occurs as a result of residual fullness below the equator line which will be unaffected by buccal fat removal. This is war of the role of peril liposuction has its benefits and contrary to the belief some there is no danger of facial nerve branch injury as non-exist in this area. As a result many patients would ideally benefit by a combined buccal lipectomy and perioral liposuction.
The role of the buccinator myoctomy in hands is limited to those patients to pose the greatest risk of getting a satisfactory soft tissue cheek reduction. These are patients that have very round face, thick tissues, and/or have been through prior soft tissue cheek reduction procedures. Much like a cheek dimple plasty it achieves its more inward soft tissue cheek contour by addressing the mucosa and muscle that lies underneath the subcutaneous fat layer.
Key Points
1) Soft tissue cheek reduction refers to the trampoline area that lies between the cheekbones and the jawline.
2) The fatty components of the soft tissue cheeks are the buccal fat pad and the subcutaneous layer both which are amenable to partial removal.
3) A relatively unknown soft tissue cheek reduction procedure is the buccinator myectomy which is a modification of the cheek dimple procedure.
4) One or all of these soft tissue cheek procedures may be needed for maximum reduction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon