

Background: The face is a set of anatomic features that structurally create a Y configuration in the middle of the face.The paired eyes/eyebrows, the vertical shaped nose that lines between them and the horizontally oriented lips or mouth that runs below the nose. Each of these 7 structures forms a facial pattern which, while quite different and variable on each face, does have certain numerical relationships between them that makes for a more or less pleasing facial appearance. These relationships between them have been studied and certain aesthetics proportions have been established.
One of the facial relationships is that of the width of the mouth, specifically the distance from one mouth corner to the other. (bi commissure distance) It has been described as being ‘golden’ if it is 1.6 that of the nostril or bialar width. The variability here lies in how aesthetically pleasing is the width of the nose so that may not be a reliable method assessment. I prefer to relate it to how it relates to the distance between the pupils of the eyes. (interpupillary distance) It is usually most ideal if the mouth width is at the same distance as a vertical line dropped down from the pupils. People who view themselves as have a small or narrow mouth will always find that the width of the mouth falls inside these vertical lines. Conversely and much more rare is those who feel their mouth is too wide/large have mouth corners that fall outside these pupillary vertical lines.
Such mouth width determinations are valuable when it comes to performing aesthetic mouth widening surgery. The amount of mouth widening needed is a measurement of how much distance is needed from the mouth corner to the vertical pupillary line. In the vast majority of patients who seek this surgery that distance varies from 3 to 7mms per side.
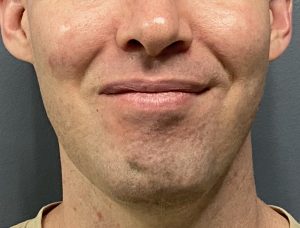
 Case Study: This male had prior facial augmentation surgeries consisting of a custom jawline and cheek implants. With a successful facial widening effect he now felt that his lips were now proportionately smaller. Even though he is smiling similar amounts in these before and after pictures it is easy to see how the mouth looks smaller in the after picture.
Case Study: This male had prior facial augmentation surgeries consisting of a custom jawline and cheek implants. With a successful facial widening effect he now felt that his lips were now proportionately smaller. Even though he is smiling similar amounts in these before and after pictures it is easy to see how the mouth looks smaller in the after picture.
 Preoperative measurements determined that the needed distance was 7mms on his left side and 6mms on the right side. A horizontal Y-V incisional pattern was marked the the V of Y along the vermilion-cutaneous borders. (he was also undergoing a sub nasal lip lift)
Preoperative measurements determined that the needed distance was 7mms on his left side and 6mms on the right side. A horizontal Y-V incisional pattern was marked the the V of Y along the vermilion-cutaneous borders. (he was also undergoing a sub nasal lip lift)

 Under sedation anesthesia the V-Y pattern of incisions were made at beach mouth corner which were of equal lengths. This creates a ‘Mercedes’ pattern with its three legs. Once the skin is incised an underlying wedge of orbicularis muscle is removed to provide space for the mouth corner to be advanced into and through.
Under sedation anesthesia the V-Y pattern of incisions were made at beach mouth corner which were of equal lengths. This creates a ‘Mercedes’ pattern with its three legs. Once the skin is incised an underlying wedge of orbicularis muscle is removed to provide space for the mouth corner to be advanced into and through.
 It also requires small triangles of skin to be removed in the corner movement outward to prevent it form looking too narrow or like a slit. The once Y pattern is now closed as a larger V.
It also requires small triangles of skin to be removed in the corner movement outward to prevent it form looking too narrow or like a slit. The once Y pattern is now closed as a larger V.

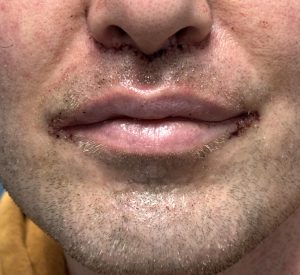 The immediate effects of the mouth widening are apparent with small 6-0 plain sutures used for the skin ciosure…so no future suture removal is needed. (there are deeper suture layers)
The immediate effects of the mouth widening are apparent with small 6-0 plain sutures used for the skin ciosure…so no future suture removal is needed. (there are deeper suture layers)
Mouth widening is an effective procedure that uses traditional plastic surgery tissue rearrangement techniques. The Mercedes incision pattern is the starting point but muscle removal and small triangles of skin removal are needed to allow the new mouth corner to be properly shaped. There will be small scar lines at the vermilion-cutaneous borders and the long term question is only how well the scar heals and whether future scar revision will be needed.
Key Points
1) The set point for mouth widening is usually out to the vertical pupillary line.
2) The Y-V technique initially creates a Mercedes incisional pattern.
3) Some orbicularis muscle removal and side skin removal is necessary for a adequately wide recreated mouth corner with a low rate of any significant relapse.
Dr. Barry Eppley
World-Renowned Plastic Surgeon