

Background: Structural waist narrowing surgery specifically refers to modification of the surrounding ribs in a manner that allows the abdominal wall musculature to collapse inward. This typically is used for the lower free floating ribs #11 and #12 since their unattached distal ends only have musculoligamentous attachments to their cartilaginous tips. The best candidates for the procedure are those patients who either are very lean and no standard body contouring procedures can be used or those patients who have already exhausted procedures that address excessive fat and skin removal around the waistline.
There are two methods to create these lower rib modifications, removal or fracture (osteotomy), for which the effectiveness differences between the two can be debated and have never been directly compared. But it would be fair to say that bony rib removal achieves maximum waist narrowing since the ligamentous attachments are fully released albeit with a more invasive surgery and a longer recovery time. Surgical access for the procedure is typically done through a small incision oriented in an oblique skin crease centered over the lateral aspect of rib #11. (Type 1 rib removal)
Such lower rib modifications can also be done for rib #10 even though it is not a true free floating rib . It does wrap around the side to the subcostal ribcage but actually does not have an attachment to it as the end of rib #10 is really free floating. As a result rib removals can include rib#10 as well with a higher level of waistline narrowing. While rib #10 can be reached from the oblique back incision it is more effectively done from a lateral torso vertical incision. (Type 2 rib removal)
But if one wants to go higher than rib#10 could rib #9 be treated as well? Not being a free floating rib with a more substantial attachment to the bottom of the subcostal ribcage a different approach needs to be taken.
 Case Study: This female had a prior Type 2 rib removal procedure with removal of the outer portions of ribs #11 and #12 as well as a segment of rib #10 through a lateral vertical torso incisions. As part of her rib removal procedure flank liposuction and latissimius dorsi muscle removal was also done. She had good improvement in a reduction of her waistline/lower torso shape.
Case Study: This female had a prior Type 2 rib removal procedure with removal of the outer portions of ribs #11 and #12 as well as a segment of rib #10 through a lateral vertical torso incisions. As part of her rib removal procedure flank liposuction and latissimius dorsi muscle removal was also done. She had good improvement in a reduction of her waistline/lower torso shape.

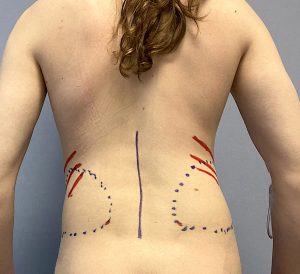
 The vertical torso scars healed very well in an almost imperceptible manner.
The vertical torso scars healed very well in an almost imperceptible manner.
Despite these good improvements she desired further narrowing higher up along the waistline. Due to the anatomy of the false ribs and their cartilaginous attachments to the anterior subcostal ribcage and sternum resection like is done in the lower ribs would leave two obvious blunt end cuts of the rib. Thus the strategy was to remove a segment of any ribs treated above rib #10 and pull the two ends together with plate fixation to extend the narrowing effect more superiorly.
 Under general anesthesia and through her existing lateral torso incisional scar the previously cut end of rib #10 was identified and another 5cm of bony rib removed.
Under general anesthesia and through her existing lateral torso incisional scar the previously cut end of rib #10 was identified and another 5cm of bony rib removed.
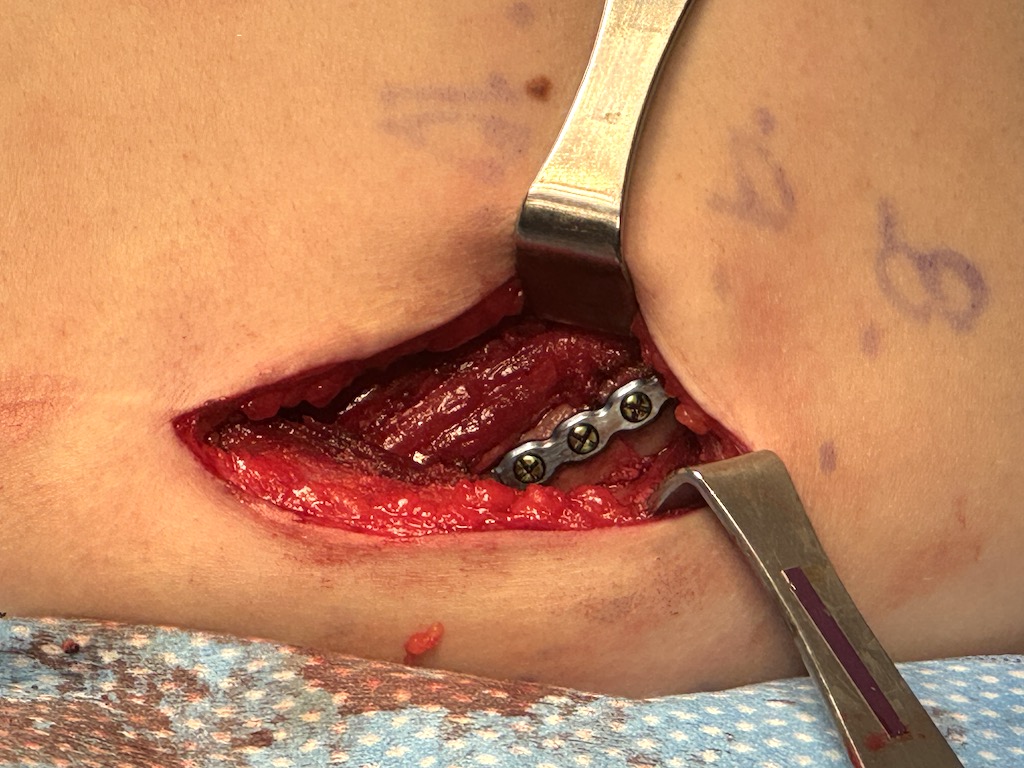
 Rib #9 was then exposed and an osteotomy cut made with a reciprocating saw. Once cut the rib ends overlapped with the distal segment falling inside the proximal segment.
Rib #9 was then exposed and an osteotomy cut made with a reciprocating saw. Once cut the rib ends overlapped with the distal segment falling inside the proximal segment.

 A cm of proximal bone was removed and and the two ends put together using a 4 hole rib plate with 8mm self tapping screws.
A cm of proximal bone was removed and and the two ends put together using a 4 hole rib plate with 8mm self tapping screws.
 The LD muscle was closed over the modified ribs and the incisions closed. No drains were used.
The LD muscle was closed over the modified ribs and the incisions closed. No drains were used.

 The addition of rib #9 length shortening added to an already good result with a further narrowing effect.
The addition of rib #9 length shortening added to an already good result with a further narrowing effect.
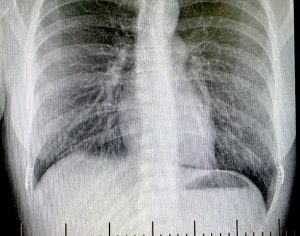 A postoeperative x-ray showed rb #9m plate fixation on each side.
A postoeperative x-ray showed rb #9m plate fixation on each side.
This case demonstrates that rib #9 can be safely and effectively reduced in length to help narrow the ribcage at an even higher level than ever done before. Because of its anatomical attachments anteriorly the lateral arc of the rib is reduced by shortening its length rather than removal or fracture. This requires rigid fixation of the two bone ends with specially designed plates for rib bone. It s possible that more than 1 cm of bone can be removed per side and may differ per patient. It is also possible that rib shortening can also be done on rib #8 for even #7 but would require a longer torso incision to do so..
Key Points
1) Lower ribcage modification for waist narrowing can be effectively done by subtotal removal of ribs #11 and #12 as they have no distal attachments.
2) Higher waist narrowing requires changes to ribs #9 and #10 for which subtotal removal of #10 can be done because of its loose cartilaginous attachment to the subcostal ribcage.
3) Modification of rib #9 requires bone resection and plate fixation for a narrowing effect.
4) Access for rib #9 and #10 is best done by a lateral torso incision oriented vertically.
Dr. Barry Eppley
World-Renowned Plastic Surgeon