

Background: There are many different types of standard facial implant styles including chin, cheek, nasal, jaw angle, tear trough/infraorbital, temporal and paranasal. Of all these off-the-shelf implant options the paranasal is unique with two distinctions. It is the smallest implant in size and probably the most infrequently used. It is also rarely in my experience requested as an independent isolated procedure. In other words it is almost never seen as the only facial implant or surgical procedure that a patient has ever had.
As the name implies the paranasal implant is a ‘nasal’ implant but not really. It is not done to enhance the nose per se but to achieve a low central midface augmentation. It does by proximity push the base of the nostrils forward but that is not a true nasal augmentation effect. It is probably better described as a pyriform aperture or even a nasolabial fold implant which more aptly describes its facial effect. The history of its use is as an adjunct to rhinoplasty particularly in the Asian patient. But today it is done more frequently as part of an overall midface skeletal augmentation concept.
Paranasal implants are available in a variety of materials with some slight differences in their sizes and shapes. The different materials from which they are made (silicone, Medpor, ePTFE) are the biggest differences between them. These different materials influence how easily they are surgically placed, able to be intraoperatively modified and secured into their desired position.
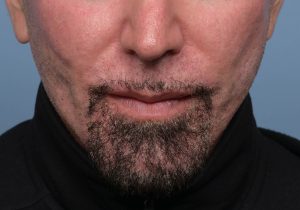
Case Study: This male had a prior aesthetic facial surgery history of custom cheek and chin implants. Because of the profound effects of these implants the central midface looked recessed by comparison. As an older male he had developed deeper nasolabial folds. Hence the desire for paranasal augmentation.

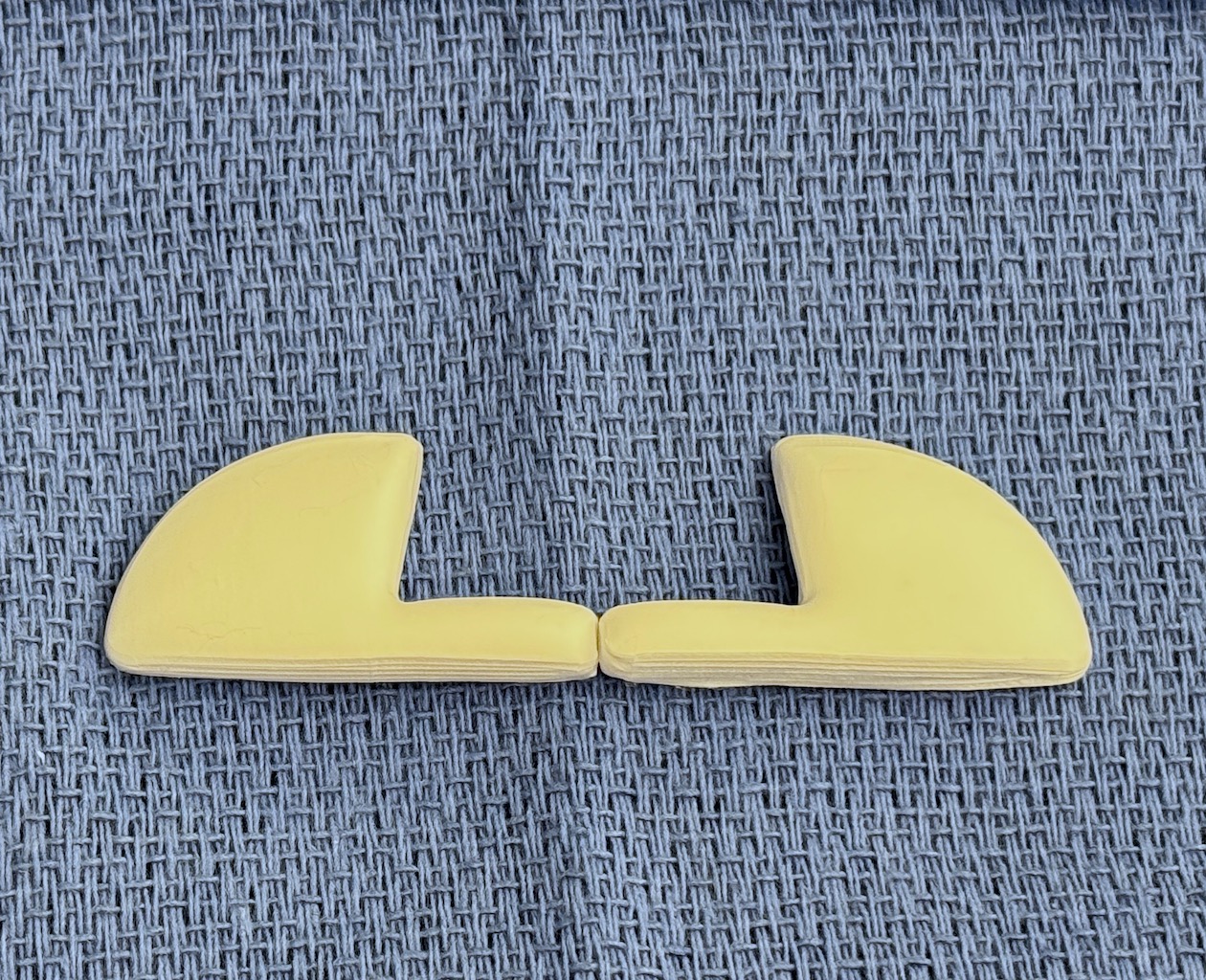
 ePTFE paranasal implants of 6mm thickness was selected which is my current preferred material for paranasal implants. The material is easily modified/carved in surgery and pass easily through small mucosal incisions underneath the nostrils. Suboperiosteal implant pockets were developed along the pyriform aperture being careful to not violate the nasal mucosa. The implants were inserted into the prepared pockets, covered with Vancomycin antibiotic powder and closed with a two layer musculomucosal closure.
ePTFE paranasal implants of 6mm thickness was selected which is my current preferred material for paranasal implants. The material is easily modified/carved in surgery and pass easily through small mucosal incisions underneath the nostrils. Suboperiosteal implant pockets were developed along the pyriform aperture being careful to not violate the nasal mucosa. The implants were inserted into the prepared pockets, covered with Vancomycin antibiotic powder and closed with a two layer musculomucosal closure.


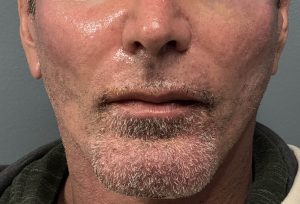 His immediate results showed the increased projection of the nasal base and softening of the nasal half of the nasolabial folds.
His immediate results showed the increased projection of the nasal base and softening of the nasal half of the nasolabial folds.
Key Points
1) The desire for paranasal augmentation is often triggered by other facial changes/surgeries.
2) Different materials exist for paranasal implants but ePTFE creates some degree of soft tissue adhesion, is easily modified intraoperatively and does not require screw fixation.
3) Small paired intraoral incisions are used for paranasal implant placement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon