

Background: The flatter midface has a long history of being treated by the LeFort I advancement bony procedure. While effective for improving projection of the upper lip, teeth and nasal base as well as improving the dental interdigitation it leaves behind the the midface structures that lie above the bone cut.This means the infraorbital rim and anterior zygomatic body (cheek) remains where they were before the surgery. This can create a new type of midface deficiency or magnify a pre-existing one.
This is particularly relevant in certain ethnic faces which have a propensity for a flatter midface profile. But in contemporary double jaw surgery (DJS), where large maxillomandibular advancements for obstructive sleep apnea or improving the skeletal projection of the lower half of the face for aesthetic purposes are done, a whole new type of aesthetic midface deformities are being created.
In improving an infraorbital-malar deficiency the only effective treatment are custom implant designs. Synthetic filler or fat injections are not going to be effective nor are any type of standard facial implant. The unique shape and differing amounts of projection needed along this arc of the upper midface, as well as the thin tissues overlying the lower eyelids and cheeks, need a precise shape to look natural.
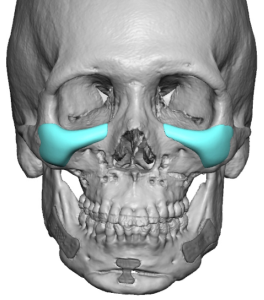
 Case Study: This male desired to improve the shape around lower eyelids and cheeks after undergoing DJS advancements and custom PEEK infraorbital-malar implants. The PEEK implants stood out unnaturally like a bump. In looking at his implant designs it was clear to me that how they looked was completely predictable given their design and their method of intraoral placement.
Case Study: This male desired to improve the shape around lower eyelids and cheeks after undergoing DJS advancements and custom PEEK infraorbital-malar implants. The PEEK implants stood out unnaturally like a bump. In looking at his implant designs it was clear to me that how they looked was completely predictable given their design and their method of intraoral placement.
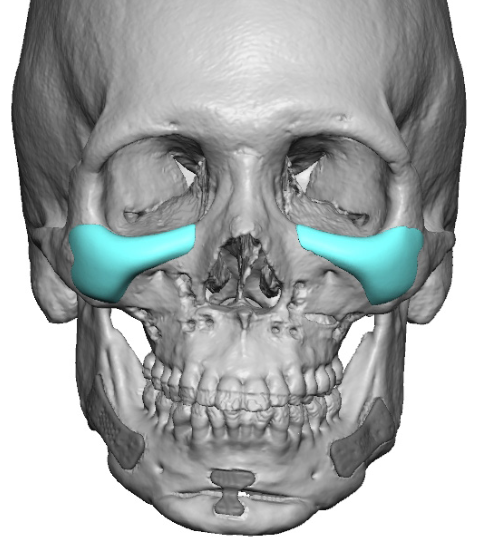
 New custom infraorbital-malar implants were designed that overcame the deficiencies of the original implant design. This was a saddle type design that fit up over and onto the infraorbital rims, less projection around the curve of the cheeks and more feathered implant edging.
New custom infraorbital-malar implants were designed that overcame the deficiencies of the original implant design. This was a saddle type design that fit up over and onto the infraorbital rims, less projection around the curve of the cheeks and more feathered implant edging.
In essence a improved and more natural Ogee curve implant design was created.

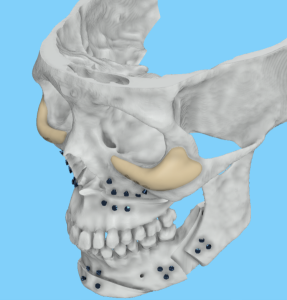
 Under general anesthesia and initially through an intraoral approach the screws through the PEEK implants were removed. (Screws almost always have to be removed through the same approach by which they were initially placed) Then through lower eyelid incisions the PEEK implants were exposed and it could be seen that the implants created anterior projection to the infraorbital rim but did not cover them. This creates a stepoff between the implant and the bone. (Hence their bump like appearance) The implants were removed and their unnatural more square cheek shape could be appreciated from above.
Under general anesthesia and initially through an intraoral approach the screws through the PEEK implants were removed. (Screws almost always have to be removed through the same approach by which they were initially placed) Then through lower eyelid incisions the PEEK implants were exposed and it could be seen that the implants created anterior projection to the infraorbital rim but did not cover them. This creates a stepoff between the implant and the bone. (Hence their bump like appearance) The implants were removed and their unnatural more square cheek shape could be appreciated from above.
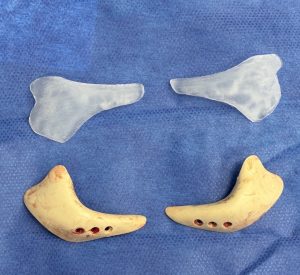
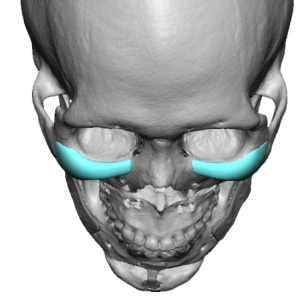
 In comparing the existing vs new custom implant designs their differences could be appreciated. In looking at their two shapes, as should be done in looking at a preoperative design, which one is going to look more natural and fit the bone in a more confluent fashion.
In comparing the existing vs new custom implant designs their differences could be appreciated. In looking at their two shapes, as should be done in looking at a preoperative design, which one is going to look more natural and fit the bone in a more confluent fashion.

 The new custom silicone infraorbital-malar implants were implanted and secured with a single micro screw. The placement shows a less pronounced implant profile with a more smoother transition into the bone.
The new custom silicone infraorbital-malar implants were implanted and secured with a single micro screw. The placement shows a less pronounced implant profile with a more smoother transition into the bone.
Bulky implant designs may be effective and not unnatural looking along the jawline due to the thicker soft tissue cover (masseter and mentalis muscles). But in the thinner tissues of the lower eyes and cheeks such implant designs are destined to look overdone and often create unnatural bone contours. Along the infraorbital rim the key to any implant design is that it almost always has to cross over onto the bony rim (saddle design). More complete infraorbital rim augmentation needs to be thought of as a 3D design (horizontal and vertical) not a 2D design. (horizontal only)
In some cases I think surgeons create implant designs based on how they plan to insert them. In this case due to the DJS the plan was obviously to place the implants with the same approach. A saddle implant design would have been much more difficult to place from an inferior approach around the infraorbital nerve. But I suspect this was more of a matter of incisional access convenience and the concept of how to do a more natural IOM implant design was simply not known.
Key Points
1) Infraorbital-malar deficiencies are not uncommon after significant LeFort I advancements.
2) Custom IOM implants are the only effective approach for bring the upper midface into balance/proportion of the lower midface.
3) The implant design and placement along the orbital rim and anterior cheek will determine if it looks natural and provides adequate upper midface correction.
Dr. Barry Eppley
World-Renowned Plastic Surgeon