


Background: One every common aesthetic facial concern is underrate hollowing. This is a general term and differs based on a congenital or aging created deficiency. A congenital under eye problem is a bony deficiency (lack of forward growth projection) while an age-related under eye problem is usually soft tissue related (fat atrophy). In the severest of cases a congenital under eye issue can be exacerbated in severity as one ages.
One defining aspect of a skeletal deficiency in a young under eye hollowing patient is the presence of a negative orbital vector. This well known assessment seen in profile view is when the cornea of the eye sticks out further than the projection of the infraorbital rim. It is the sine qua non of an infraorbital rim deficiency. There is usually excessive scleral show due to lid retraction and there may be some dry eye symptoms as well. On thorough ophthalmologic examination corneal changes may also be present.
In the negative orbital vector patient the definitive improvement comes from skeletal augmentation. Synthetic fillers and fat injections may be tried but they will ultimately be unsatisfactory. Soft tissue volume simply does not provide enough push or augmentation effect. But in using implants its footprint must essentially be that of an infraorbital-lateral orbital rim skeletal expansion effect. To correct a bone problem the implant should create a skeletal expansion effect…expand the natural bony contours as if that was the way they were intended to develop. This is why any form of a standard implant, what I call a spot augmentation, is simply inadequate. This is the benefit of a custom implant design in the negative orbital vector patient.
While an implant addresses the bony deficiency and helps drive up the lower eyelid to some degree, direct lengthening of the lower eyelid via spacer grafts is a great addition to what the effect of a custom infraorbital-malar (IOM) implant can achieve.

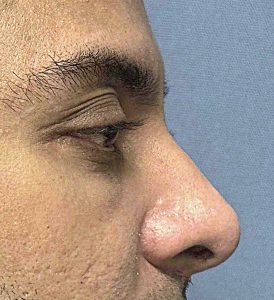
 Case Study: This young male had infraorbital rim-malar recession with excessive scleral show and dry eyes. As a result he had pseudo orbital proptosis. (Bulging eyes but not due to the eyes actually being too protrusive) Custom infraorbital-lateral orbital implants were designed and placed through lower eyelid incisions.
Case Study: This young male had infraorbital rim-malar recession with excessive scleral show and dry eyes. As a result he had pseudo orbital proptosis. (Bulging eyes but not due to the eyes actually being too protrusive) Custom infraorbital-lateral orbital implants were designed and placed through lower eyelid incisions.
![]() At the same time lower eyelid spacer grafts were placed (medium thickness Alloderm) between the tarsus superiorly and the orbicularis muscle inferiorly.
At the same time lower eyelid spacer grafts were placed (medium thickness Alloderm) between the tarsus superiorly and the orbicularis muscle inferiorly.

 When seen nearly one year later the improvement in lower orbital projection and lower eyelid position was very evident. The amount of scleral show was reduced and the severity of his dry eye symptoms reduced. (Notice that I said reduced not eliminated)
When seen nearly one year later the improvement in lower orbital projection and lower eyelid position was very evident. The amount of scleral show was reduced and the severity of his dry eye symptoms reduced. (Notice that I said reduced not eliminated)

 When it comes to the negative orbital vector patient the anatomic problem is of a combined hard and soft tissue composition. Combining lower orbital skeletal expansion and soft tissue lower eyelid lengthening is the most effective approach. The use of contemporary custom implant designing with lower eyelid soft tissue lengthening offers the patient the best chance for improvement. And as this case shows any dry eye symptoms should show some signs of improvement.
When it comes to the negative orbital vector patient the anatomic problem is of a combined hard and soft tissue composition. Combining lower orbital skeletal expansion and soft tissue lower eyelid lengthening is the most effective approach. The use of contemporary custom implant designing with lower eyelid soft tissue lengthening offers the patient the best chance for improvement. And as this case shows any dry eye symptoms should show some signs of improvement.
Key Points:
1) The negative orbital vector can be improved by a custom IOM implant design through periorbital bony expansion.
2) A lower eyelid spacer graft can be a good addition to the custom IOM implant to help drive up the lower eyelid position.
3) In the dry eye negative orbital vector patient some reduction in corneal irritation can usually be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon