


Background: Rhinoplastyis an operation capable of making multidimensional changes to the shape of the nose. Through an individualized series of augmentative and reduction techniques the osteocartilaginous framework is altered and the final result seen when the overlying skin has fully wrapped around and adhered tightly to this new shape. Thus in planning each patient’s rhinoplasty surgery various techniques are considered in how affect each desired dimensional shape change.
While each patient’s nose shape and rhinoplasty surgery are unique there are some basic nose shapes where the combination of techniques used are fairly uniform. One such example is the underdeveloped nose where the bridge is low and the tip is wide. Techniques needed are bridge augmentation and tip reduction/narrowing. With these technique concepts are what type of material or graft is needed for the augmentation with the classic debate of an implant vs a rib graft to perform it. This is not really a debate rather its requires an understanding of the advantages or disadvantages of each augmentation approach.
Similarly for narrowing the tip of the nose the consideration is whether the nostrils should be narrowed as the bridge is elevated and the tip cartilages are narrowed. If so should the nostrils be narrowed by internal wedge or alar base resection.
Case Study: This make desired a change in the shape of his nose which had an underdeveloped bridge, wide nasal bones, broad nasal tip and flared nostrils. The plan was for dorsal augmentation, low to low nasal bone osteotomies, tip cartilage narrowing by cartilage resection and suturing and nostril narrowing.

 Under general anesthesia and through an open approach the bridge was augmented by a solid silicone implant of 7mm height and 40mms in length.
Under general anesthesia and through an open approach the bridge was augmented by a solid silicone implant of 7mm height and 40mms in length.

 In placing a nasal implant it is the higher broader end that is placed at the nasofrontal junction and the narrow lower end behind/under the cephalic margin of the lower alar cartilages. Almost always the lower end needs to be tapered to not create undesired supra tip fullness. Such tapering also allows for the end of the implant to fit snugly under the lower alar cartilages. Once the nasal implant was placed the tip cartilage reshaping was done to thin and narrow them with cephalic margin resection (6mm) double dome suturing, lateral crural spanning sutures and tip grafting.
In placing a nasal implant it is the higher broader end that is placed at the nasofrontal junction and the narrow lower end behind/under the cephalic margin of the lower alar cartilages. Almost always the lower end needs to be tapered to not create undesired supra tip fullness. Such tapering also allows for the end of the implant to fit snugly under the lower alar cartilages. Once the nasal implant was placed the tip cartilage reshaping was done to thin and narrow them with cephalic margin resection (6mm) double dome suturing, lateral crural spanning sutures and tip grafting.
The nasal skin was then closed and low to low nasal bone osteotomies performed.

 Lastly nostril narrowing was performed with 4mm internal wedge resections.
Lastly nostril narrowing was performed with 4mm internal wedge resections.

 The immediate intraop changes in the nose were apparent at the end of the procedure.
The immediate intraop changes in the nose were apparent at the end of the procedure.
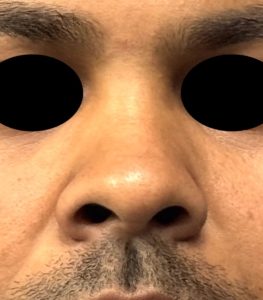
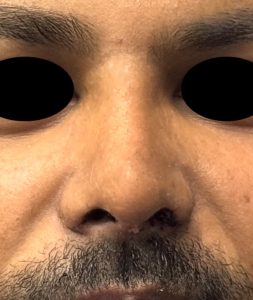
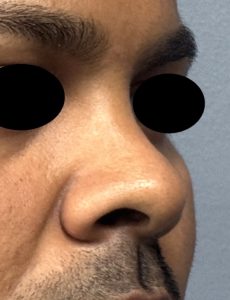
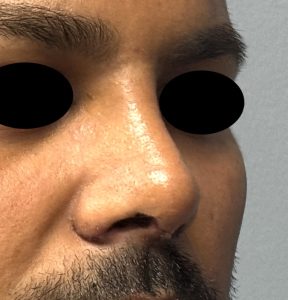 At removal of the nasal splint and tapes on week later the three dimensional effect of the overall rhinoplasty surgery could be better seen (even though it can take up to a full year to see the complete thinning effect).
At removal of the nasal splint and tapes on week later the three dimensional effect of the overall rhinoplasty surgery could be better seen (even though it can take up to a full year to see the complete thinning effect).
The use of combined dorsal line augmentation with reductive bone osteotomes, cartilage excision/reshaping/grafting and skin removal (nostril narrowing) is a synergistic surgery of which each component contributes to the final result through diametric changes. It is hard to say any one component is more important than the other but the significant dorsal line or bridge augmentation probably makes a bit more change than any one of the other elements. In considering that augmentation the use of a implant provides an immediate and sustained effect that assures having a smooth dorsal line contour that is straight. While it is an implant which does carry its own risk of infection that risk is reduced when it is placed through an open approach which avoids direct intranasal mucosal exposure.
Key Points:
1) Rhinoplasty for the wide saddle shaped nose requires a multidimensional approach of dorsal augmentation and tips and nostril narrowing.
2) A nasal implant is a reliable method for dorsal augmentation that provides an assured smooth contour and predictable height increases.
3) Nostril narrowing is often necessary when an overall thinner nasal shaped is desired.
Dr. Barry Eppley
World-Renowned Plastic Surgeon