

 The width of the side of the head through subtotal temporal muscle removal has proven to be a consistently safe and effective aesthetic procedure. A common and understandable question from patients is whether this type of muscle reduction might impair jaw function or chewing. It seems logical to assume that removing a portion of a muscle involved in mastication would cause such issues. However, after performing this surgery hundreds of times, no such adverse effects have been observed.
The width of the side of the head through subtotal temporal muscle removal has proven to be a consistently safe and effective aesthetic procedure. A common and understandable question from patients is whether this type of muscle reduction might impair jaw function or chewing. It seems logical to assume that removing a portion of a muscle involved in mastication would cause such issues. However, after performing this surgery hundreds of times, no such adverse effects have been observed.
Anatomy of the Temporal Muscle
Traditionally depicted in anatomical texts as a single muscle layer, the temporalis muscle originates broadly along the bony temporal line. It narrows as it travels beneath the zygomatic arch to attach to the coronoid process of the mandible. More recent anatomical studies have clarified that the temporalis is actually composed of two distinct layers—a superficial and a deep part—each inserting at different sites on the mandible.
-
The superficial portion is the more prominent, fan-shaped muscle visible externally, inserting at the lateral retromolar area.
-
The deep portion is narrower, more vertically oriented, and inserts on the medial aspect of the retromolar triangle.
Because temporal reduction surgery primarily targets the superficial layer, the deeper segment remains intact. Moreover, even the superficial portion is only partially removed in most cases. This preservation of function explains why mastication and jaw movement remain unaffected postoperatively.
Case Study
 A young male patient presented with an unusually wide head due to hypertrophy of the temporal muscles. Interestingly, his muscle fullness was concentrated in the upper, posterior segment—more so than the anterior portion, which is an uncommon presentation in my experience.
A young male patient presented with an unusually wide head due to hypertrophy of the temporal muscles. Interestingly, his muscle fullness was concentrated in the upper, posterior segment—more so than the anterior portion, which is an uncommon presentation in my experience.

![]() Surgery was performed under general anesthesia through a high postauricular incision. The posterior temporal muscle was detached from the overlying fascia superiorly and the bone inferiorly. A high release along the temporal line, extending halfway down the forehead, allowed the muscle to be mobilized and delivered through the incision.
Surgery was performed under general anesthesia through a high postauricular incision. The posterior temporal muscle was detached from the overlying fascia superiorly and the bone inferiorly. A high release along the temporal line, extending halfway down the forehead, allowed the muscle to be mobilized and delivered through the incision.
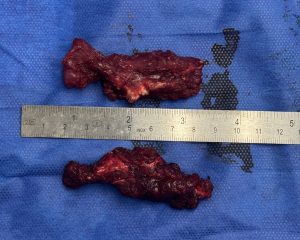
 The transposed muscle was partially excised, and the remaining portion was secured to a cuff of deep temporal fascia using a combined removal and transposition technique. The incisions were closed with resorbable sutures, and no drains were needed.
The transposed muscle was partially excised, and the remaining portion was secured to a cuff of deep temporal fascia using a combined removal and transposition technique. The incisions were closed with resorbable sutures, and no drains were needed.

 The aesthetic improvement was immediately evident upon closure.
The aesthetic improvement was immediately evident upon closure.
Discussion on Surgical Techniques
Temporal muscle reduction can be performed via:
-
Muscle removal, which typically targets the portion of the muscle that covers the convexity of the temporal bone.
-
Muscle transposition, ideal for addressing anterior muscle bulk located in the concavity of the deep temporal fossa.
-
A combination approach, used in cases requiring broader contour refinement.
In many patients, removing the posterior muscle bulk is sufficient. However, in others with hypertrophy extending into the anterior temporal region, direct removal is not feasible via a postauricular incision and may leave a noticeable cut-edge deformity. In these cases, transposition is preferred to contour the anterior muscle while preserving a smooth surface appearance.
Even with transposition, the lowermost anterior muscle region remains difficult to access. Fortunately, in this particular case, reduction in that area was unnecessary.
Key Points
-
Temporal muscle hypertrophy is a recognized cause of an overly convex or wide side-of-head appearance.
-
Muscle reduction may be achieved through excision, transposition, or both, depending on the anatomic presentation.
-
These techniques do not impair jaw function or chewing in the long term.
Dr. Barry Eppley
World-Renowned Plastic Surgeon