


Background
Patients seeking facial width reduction are usually focused on the cheeks, which are typically the widest part of the face. This width is primarily due to the zygomatic arch, which must curve outward to allow the temporal muscle to pass beneath it and attach to the ramus of the lower jaw. To narrow facial width, the arch of the cheekbone must be repositioned inward. This is achieved through anterior and posterior osteotomies; simple bone shaving is ineffective because the bone is too thin and not easily accessible.
There are several osteotomy patterns used in cheekbone reduction surgery. The greatest variability lies in the anterior arch where it meets the zygomatic major, as the thicker bone allows for different approaches. Commonly used patterns include oblique and L-shaped osteotomies, each with distinct advantages and drawbacks. At the posterior arch, however, the bone is so thin and narrow that only a straight-line cut is feasible.
The oblique osteotomy is the original technique. Historically, it was performed without rigid fixation, which led to bone and soft tissue sagging as well as visible step-offs through the cheekbone. More geometric bone cut designs have helped eliminate these issues, though refinements in technique continue to improve outcomes.
Case Study
This young male had previously undergone a sliding genioplasty and desired additional facial reshaping through cheek narrowing. His goal was to reduce the width of the mid-zygomatic arch so that it aligned with the temporal areas above it.

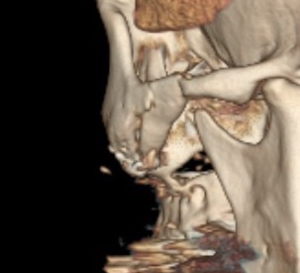
 Under general anesthesia, intraoral incisions were made, and a reciprocating saw was used to perform a full-thickness cut from the posterior zygomatic buttress to the lateral orbital rim. This cut alone, however, would not mobilize the cheekbone. To achieve inward movement, a 7mm vertical incision was placed inside the sideburn hairline. Through this incision, a double cut (two osteotomies spaced 1 cm apart) was performed on the posterior zygomatic arch, allowing the bone to shift inward smoothly without creating a step-off or requiring plate fixation.
Under general anesthesia, intraoral incisions were made, and a reciprocating saw was used to perform a full-thickness cut from the posterior zygomatic buttress to the lateral orbital rim. This cut alone, however, would not mobilize the cheekbone. To achieve inward movement, a 7mm vertical incision was placed inside the sideburn hairline. Through this incision, a double cut (two osteotomies spaced 1 cm apart) was performed on the posterior zygomatic arch, allowing the bone to shift inward smoothly without creating a step-off or requiring plate fixation.
 The anterior cheek osteotomy was beveled at a 45-degree angle to prevent a visible/palpable step off. The mobilized bone segment was moved inward by 8mm and secured with plate fixation to counteract the downward pull of the masseter muscle.
The anterior cheek osteotomy was beveled at a 45-degree angle to prevent a visible/palpable step off. The mobilized bone segment was moved inward by 8mm and secured with plate fixation to counteract the downward pull of the masseter muscle.

 At the completion of the procedure, the immediate cheek narrowing was evident.
At the completion of the procedure, the immediate cheek narrowing was evident.
Discussion
 Cheekbone reduction osteotomies have evolved to include various bone cut patterns, particularly at the junction of the zygomatic arch and zygomatic major. The L-shaped osteotomy provides a more three-dimensional reshaping, allowing some rotation and offering greater bone contact for healing. In contrast, the oblique osteotomy is a two-dimensional reduction with less healing surface, though it provides adequate stability for pure width reduction.
Cheekbone reduction osteotomies have evolved to include various bone cut patterns, particularly at the junction of the zygomatic arch and zygomatic major. The L-shaped osteotomy provides a more three-dimensional reshaping, allowing some rotation and offering greater bone contact for healing. In contrast, the oblique osteotomy is a two-dimensional reduction with less healing surface, though it provides adequate stability for pure width reduction.
 The double osteotomy at the posterior zygomatic arch allows for stable inward repositioning without the need for hardware fixation. This approach reduces scar size and lowers the risk of injuring the frontal branch of the facial nerve.
The double osteotomy at the posterior zygomatic arch allows for stable inward repositioning without the need for hardware fixation. This approach reduces scar size and lowers the risk of injuring the frontal branch of the facial nerve.
Key Points
-
Cheekbone reduction requires both anterior and posterior osteotomies, which together enable complete infracture of the zygomatic arch.
-
The degree of possible reduction depends on the natural shape of the arch; more convex arches allow greater inward repositioning.
-
The oblique osteotomy, though an older technique, remains effective when combined with plate fixation and a corner osteotomy.
Dr. Barry Eppley
World-Renowned Plastic Surgeon