

Background
Two types of surgery often create a subsequent need for custom facial implants: facial feminization surgery (FFS) and double jaw surgery (DJS). DJS effectively repositions the lower midface and jaw, but significant forward movements can leave the upper midface behind, creating undereye hollowing and cheek deficiencies. These effects are magnified if preexisting midface deficiencies were already present. Custom infraorbital and infraorbital-malar implants are optimal for addressing these surgically induced concerns.
In FFS, one of the main procedures is brow bone reduction, often performed with a bone flap or Type III technique. The lateral (tail) portion of the brow bone is typically reduced by bone burring, softening a masculine appearance. However, a small percentage of patients later choose to de-transition and seek to remasculinize their face. In such cases, brow bone augmentation is required and is best accomplished with a custom implant.
Combining brow bone and infraorbital-malar implants allows for circumferential periorbital augmentation, particularly relevant for patients who have undergone both FFS and DJS. These implant designs are straightforward to create from a 3D CT scan, though accurate placement with limited incisional access can be technically challenging.
Patient Case
 This patient had previously undergone both DJS and FFS. As part of the DJS, custom Medpor orbital rim implants were placed intraorally, but they led to edge visibility and worsened undereye hollowing postoperatively. Because Medpor is not visible on CT scans, only the fixation screws could be identified. During FFS, brow bone reduction was performed with burring, causing collapse of the outer bone layer into the frontal sinus and resulting in bilateral concave depressions.
This patient had previously undergone both DJS and FFS. As part of the DJS, custom Medpor orbital rim implants were placed intraorally, but they led to edge visibility and worsened undereye hollowing postoperatively. Because Medpor is not visible on CT scans, only the fixation screws could be identified. During FFS, brow bone reduction was performed with burring, causing collapse of the outer bone layer into the frontal sinus and resulting in bilateral concave depressions.
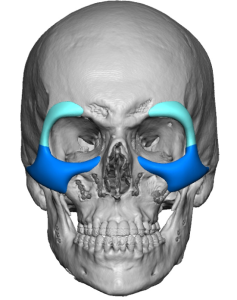
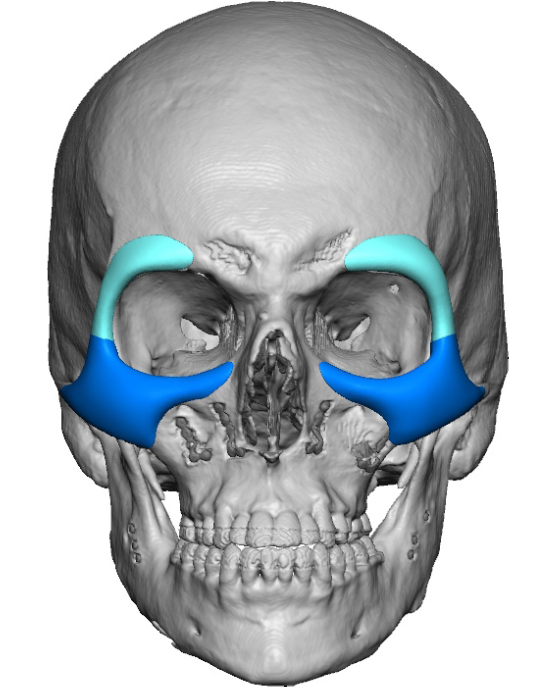
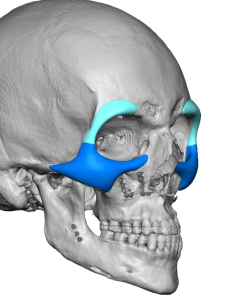
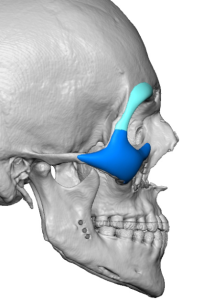 The patient sought restoration of his brow bones and more natural infraorbital and cheek augmentation without edging. Since the medial brow bone was exposed to the frontal sinus, an implant could not be placed there. Although bone cement was considered, the patient declined re-opening the forehead flap. Injectable fillers were planned for the medial brow, while custom implants were designed for the lateral brow and infraorbital-malar regions. These designs were created as two-piece implants per side, seamlessly connected around the periorbital area.
The patient sought restoration of his brow bones and more natural infraorbital and cheek augmentation without edging. Since the medial brow bone was exposed to the frontal sinus, an implant could not be placed there. Although bone cement was considered, the patient declined re-opening the forehead flap. Injectable fillers were planned for the medial brow, while custom implants were designed for the lateral brow and infraorbital-malar regions. These designs were created as two-piece implants per side, seamlessly connected around the periorbital area.
Surgical Approach

 Under general anesthesia, the Medpor orbital rim implants and their fixation screws were removed via the original intraoral approach. The removed implants were compared to the custom replacements. The Medpor implants were small, localized “spots” on the bone, while the custom implants featured broader surface coverage, resembling natural bone contours.
Under general anesthesia, the Medpor orbital rim implants and their fixation screws were removed via the original intraoral approach. The removed implants were compared to the custom replacements. The Medpor implants were small, localized “spots” on the bone, while the custom implants featured broader surface coverage, resembling natural bone contours.


 Incisions were made in the lower eyelid (subciliary) and upper eyelid crease. Through the upper eyelid incision, the lateral brow bone implant was positioned just short of the supraorbital nerve and fixed to the lateral orbital rim with a microscrew. The larger infraorbital-malar implant was introduced via the lower eyelid incision and connected end-to-end with the brow implant. It was secured to the infraorbital rim and cheekbone with two microscrews.
Incisions were made in the lower eyelid (subciliary) and upper eyelid crease. Through the upper eyelid incision, the lateral brow bone implant was positioned just short of the supraorbital nerve and fixed to the lateral orbital rim with a microscrew. The larger infraorbital-malar implant was introduced via the lower eyelid incision and connected end-to-end with the brow implant. It was secured to the infraorbital rim and cheekbone with two microscrews.
Technical Considerations
 Implant placement around the orbital rims presents unique challenges. The implants must have feathered edges and smooth contours to blend naturally with the thin eyelid tissues. Poorly designed or edged implants risk visibility, making custom silicone implants ideal, as only silicone can achieve truly feathered edges. This explains higher dissatisfaction rates with other materials.
Implant placement around the orbital rims presents unique challenges. The implants must have feathered edges and smooth contours to blend naturally with the thin eyelid tissues. Poorly designed or edged implants risk visibility, making custom silicone implants ideal, as only silicone can achieve truly feathered edges. This explains higher dissatisfaction rates with other materials.
Accurate implant positioning is equally important. Infraorbital components, in particular, are best placed through a lower eyelid incision. Intraoral placement makes it difficult to position implants correctly over the infraorbital rim and carries risks of infraorbital nerve stretch injury, potentially causing temporary or permanent numbness. By contrast, the lower eyelid incision avoids these risks and ensures precise placement, despite leaving a fine scar.
Key Points
- Reversing FFS often requires augmentation of previously reduced bone areas, such as the brow bone and jaw.
- Custom implant designs, guided by 3D CT scans, are the most effective method for achieving FFS reversal.
- Custom implants also help the midface maintain balance following jaw advancements.
- Custom periorbital implants can be discreetly placed through eyelid incisions, ensuring accurate positioning and natural results.
Dr. Barry Eppley
World-Renowned Plastic Surgeon