

Introduction
Modifications of the iliac crest represent one of several aesthetic skeletal contouring procedures, alongside ribcage narrowing, clavicle shortening or lengthening, and limb-length modification.
Iliac crest expansion (pelvic plasty) is a relatively new hip-widening procedure that uses a metal implant. In contrast, iliac crest reduction reduces excessive bony hip width or prominent crestal ridges. This remains a lesser-known aesthetic operation, primarily due to its rarity and low patient awareness.
Anatomy
![]()
![]()
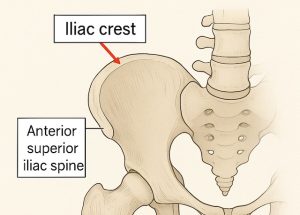 The iliac crest is the upper ridge of the ilium, extending from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS).
The iliac crest is the upper ridge of the ilium, extending from the anterior superior iliac spine (ASIS) to the posterior superior iliac spine (PSIS).
It serves as an attachment site for several muscles and fasciae, including the tensor fasciae latae and abdominal wall muscles.
In lean or athletic individuals, a prominent iliac crest can create a wider-appearing hip or an undesired upper-hip contour.
Iliac crest reduction aims to decrease this bony prominence—particularly the anterolateral portion—to create a smoother transition between the waist and hips. Typically, 8–15 mm of bone is removed from the most prominent area.
Indications
Ideal candidates are individuals with visibly or palpably prominent iliac crests (“hip wings”), particularly those with minimal subcutaneous fat who feel that the bony width disrupts their desired silhouette.
Recovery and Limitations
-
Walking may be uncomfortable for 7–10 days due to fascial attachments and bone work.
-
Return to strenuous activity typically occurs within 4–6 weeks.
-
Potential risks include visible scarring, contour irregularities, asymmetry, and rare chronic pain.
-
Limitation: Only a modest amount of bone can be safely removed; preoperative imaging is important to align expectations with achievable outcomes.
Case Study
A young, thin female presented with prominent iliac crests that projected outward between her waistline and subiliac hollows, creating an undesired silhouette. Treatment options included:
-
Augmentation of the subiliac hollows with implants, or
-
Bony reduction of the iliac crests.
She chose the latter.
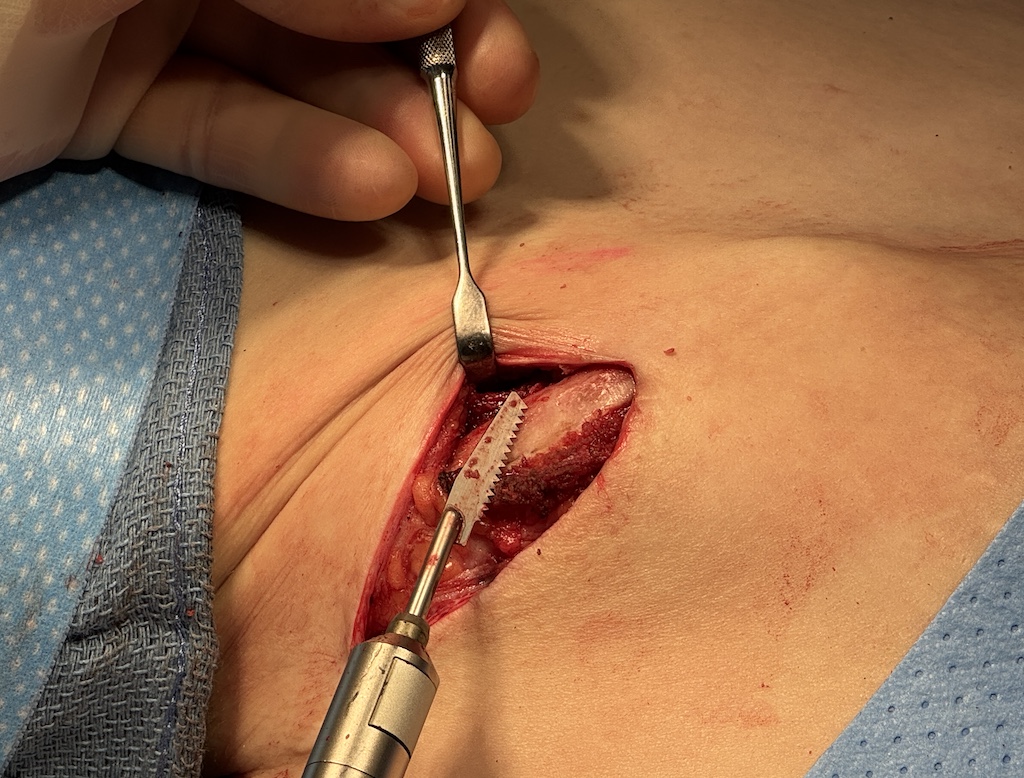
Under general anesthesia, the patient was placed supine. Typically, an incision is made just below or slightly behind the ASIS along the anterolateral crest to conceal the scar. In this case, existing scars from previous hip implant surgery were repurposed, providing convenient access.

 Dissection exposed the upper and outer iliac crest, with limited release of soft-tissue attachments (notably the tensor fasciae latae fascia). The bony ridge was reduced using a reciprocating saw, focusing on the lateral convexity responsible for excessive hip width.
Dissection exposed the upper and outer iliac crest, with limited release of soft-tissue attachments (notably the tensor fasciae latae fascia). The bony ridge was reduced using a reciprocating saw, focusing on the lateral convexity responsible for excessive hip width.

 Intraoperative comparison demonstrated a visible reduction in prominence. After contouring both crests, soft-tissue attachments were resutured, and layered closure was performed with a subcuticular finish. Drains were not required.
Intraoperative comparison demonstrated a visible reduction in prominence. After contouring both crests, soft-tissue attachments were resutured, and layered closure was performed with a subcuticular finish. Drains were not required.



 Postoperatively, the elimination of the iliac crest prominence was readily apparent within days.
Postoperatively, the elimination of the iliac crest prominence was readily apparent within days.
Discussion
Iliac crest reduction refines the waist–hip transition by diminishing the lateral bony flare without impairing pelvic or hip function. Ambulatory discomfort typically resolves within two weeks. Scarring is minimal and strategically placed below the crest.
The procedure is most effective in reducing flaring or lateral prominence rather than significantly narrowing total hip width. It should be viewed as a prominence reduction, not a major hip-narrowing operation.
Recovery highlights:
-
Downtime: 10–14 days for light activity
-
Sitting and side-lying positions are well tolerated
-
Initial gait changes (shuffling or waddling) resolve after the first week
-
Mild swelling and bruising may persist for several weeks
-
Final contour stabilizes in 2–3 months
The incision scar typically fades over several months; silicone sheeting or scar gel can optimize its appearance.
Important Considerations
-
How much width reduction is anatomically feasible, and what result can be expected?
-
What is the exact scar location and anticipated visibility?
-
How are soft-tissue attachments managed to prevent long-term weakness or pain?
-
What are the postoperative care protocols (e.g., walking restrictions, compression garments)?
-
Can this procedure be combined with other contouring surgeries?
Key Points
-
Purpose: Removal of the superolateral bony flare to create a smoother waist–hip contour.
-
Recovery: Temporary gait discomfort from minor tensor fasciae latae disruption.
-
Outcome: Permanent bony reduction with no long-term functional limitations.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon