

Introduction
Chin pad ptosis correction encompasses surgical techniques designed to elevate or remove a drooping chin soft-tissue pad. This condition most commonly results from prior chin bone reduction, chin implant surgery, or implant removal.
Etiology of Chin Pad Ptosis
Common causes include:
- Mentalis muscle detachment or laxity
(very common after chin implant removal)
- Loss of bony chin projection and structural support
- Age-related soft-tissue descent
- Chin implant malposition
Clinical Presentation
Patients may present with:
- A classic “witch’s chin” deformity
- Vertical chin wrinkling at rest
- Inferior migration of the chin soft-tissue pad
- Poor lip competence or excessive mentalis strain
Surgical Correction Options
1. Mentalis Muscle Resuspension
This is the most commonly cited and historically favored technique, although frequent use does not necessarily equate to universal appropriateness.
Technique
- Intraoral vestibular approach
- Identification of the mentalis muscle edges
- Reattachment of the muscle to one of the following:
- Chin bone (via drill holes)
- Chin implant
- Titanium micro-screws
- Chin bone (via drill holes)
- Layered closure to restore sphincter function
Indications — Tissue Laxity Problem
- Soft-tissue disinsertion
- Stretched or weakened mentalis muscle
2. Submental Chin Pad Excision / Tuck
Often described as being reserved for more “severe” cases of chin pad ptosis, this technique can be effectively applied across a wide range of severities.
Technique
- Submental incision
- Direct elevation of the chin pad
- Shortening of the mentalis muscle insertion
- Secure fixation of the chin pad to the inferior border of the chin bone
Advantages
- Powerful and predictable correction
Disadvantages
- Creation of a submental scar
- Possible need for secondary scar revision or minor residual ptosis correction
Indications — Tissue Excess Problem
- Iatrogenic bone loss (post–chin reduction surgery)
- Loss of chin projection (post–implant removal or sliding genioplasty setback)
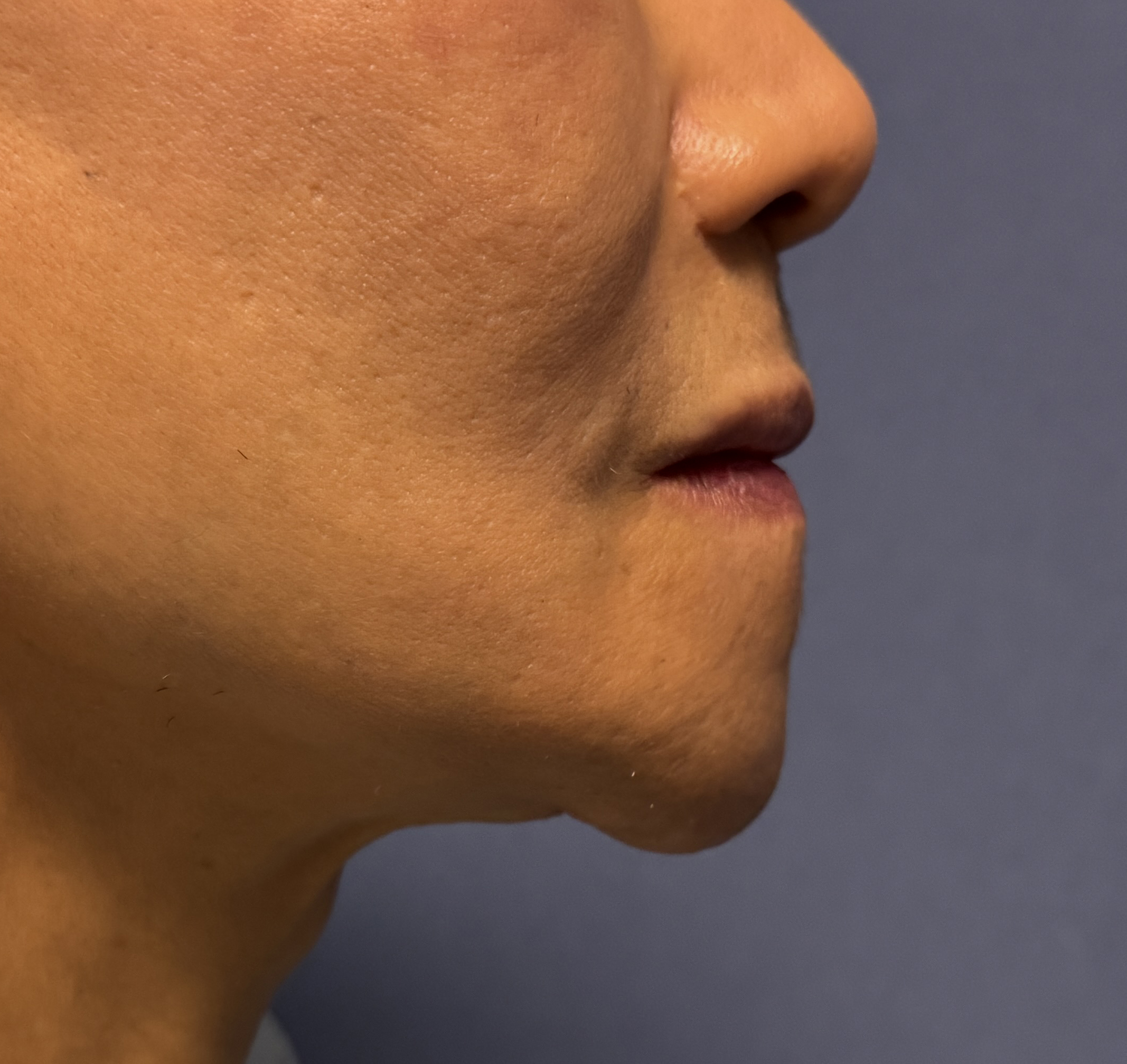
Case Study

 This female patient had previously undergone an intraoral 6-mm reduction of horizontal chin projection. This resulted in immediate inferior descent of the chin pad and development of a pronounced “witch’s chin” deformity. Subsequent attempts at correction with a facelift were unsuccessful.
This female patient had previously undergone an intraoral 6-mm reduction of horizontal chin projection. This resulted in immediate inferior descent of the chin pad and development of a pronounced “witch’s chin” deformity. Subsequent attempts at correction with a facelift were unsuccessful.
On examination, the chin pad was markedly loose and hanging. This resulted not only from release of the osteocutaneous ligaments, but also from a mismatch between the reduced bony support and the existing soft-tissue volume.


 A submental approach was performed. Elevation of the entire chin pad off the bone revealed an indwelling plate and screws, confirming that the prior reduction was performed via osteotomy rather than burring. Redundant chin pad tissue was excised, followed by a multilayer closure using resorbable sutures.
A submental approach was performed. Elevation of the entire chin pad off the bone revealed an indwelling plate and screws, confirming that the prior reduction was performed via osteotomy rather than burring. Redundant chin pad tissue was excised, followed by a multilayer closure using resorbable sutures.

 The intraoperative side profile demonstrated a significant reduction in soft-tissue chin bulk and improved chin pad positioning without pulling down the lower lip.
The intraoperative side profile demonstrated a significant reduction in soft-tissue chin bulk and improved chin pad positioning without pulling down the lower lip.
Discussion
When chin pad ptosis or a witch’s chin deformity is encountered, treatment options can be broadly divided into superior and inferior approaches. This distinction represents more than simply different access points; the underlying surgical concepts and mechanisms are fundamentally different.
The superior (intraoral) approach relies on lifting and resuspending the chin pad and is most effective when soft-tissue volume is appropriate and true excess is minimal.
In contrast, the inferior (submental) approach achieves correction primarily through tissue excision and inferior border fixation. This method works best when the chin pad is not excessively lax but is oversized relative to the reduced bony chin support.
Key Points
- Submental chin pad excision is indicated when there is a mismatch between bony chin support and soft-tissue volume, most often iatrogenic in origin.
- The submental technique combines selective tissue excision with fixation of the chin pad to the inferior border of the mandible to achieve durable correction.
Barry Eppley, MD, DMD