

Introduction
Total temporomandibular joint (TMJ) replacement is a surgical procedure in which a damaged jaw joint is replaced with a biocompatible prosthesis to relieve pain and restore function when conservative treatments have failed. It is most commonly indicated for severe degenerative joint disease, including osteoarthritis and rheumatoid arthritis, as well as advanced joint destruction, deformity, or resorption.
Modern TMJ replacements are custom-made prostheses designed from the patient’s three-dimensional CT scans. This approach allows for precise adaptation to the patient’s anatomy, improved jaw alignment, and more predictable long-term outcomes. The prosthesis consists of two components: a mandibular component that replaces the condyle and is fabricated from a titanium alloy, and a fossa component that replaces the socket and is made from ultra-high-molecular-weight polyethylene (UHMWPE).
Although TMJ replacement reliably improves joint function, it does not address pre-existing bony jaw angle asymmetry. In addition, surgical trauma can contribute to postoperative soft-tissue thinning or volume loss, which may further accentuate facial asymmetry. Correction of such asymmetry may therefore require additional custom bony implants and/or soft-tissue augmentation for optimal aesthetic improvement.
Case Study
 This older female patient previously underwent bilateral total TMJ joint replacement with significant improvement in her preoperative symptoms. Her primary residual concern was a persistent left jaw angle and lower facial asymmetry.
This older female patient previously underwent bilateral total TMJ joint replacement with significant improvement in her preoperative symptoms. Her primary residual concern was a persistent left jaw angle and lower facial asymmetry.
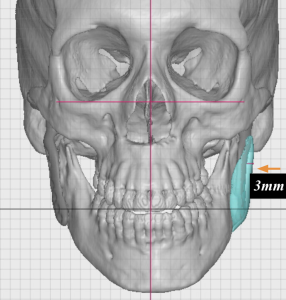
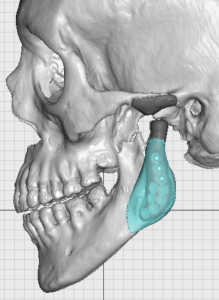 Three-dimensional CT analysis demonstrated a 3-mm width discrepancy between the two sides at the jaw angle, attributable to bony and prosthetic asymmetry. To correct this structural difference, a custom overlay jaw angle implant was designed. The facial asymmetry also had a significant soft-tissue component. Prior fat injections had been attempted but were completely resorbed. The treatment plan therefore included placement of allogeneic dermal graft onlays in a subcutaneous plane.
Three-dimensional CT analysis demonstrated a 3-mm width discrepancy between the two sides at the jaw angle, attributable to bony and prosthetic asymmetry. To correct this structural difference, a custom overlay jaw angle implant was designed. The facial asymmetry also had a significant soft-tissue component. Prior fat injections had been attempted but were completely resorbed. The treatment plan therefore included placement of allogeneic dermal graft onlays in a subcutaneous plane.
 A combined hard- and soft-tissue correction was planned, utilizing the patient’s existing preauricular incision.
A combined hard- and soft-tissue correction was planned, utilizing the patient’s existing preauricular incision.
 A plastic model of the custom jaw angle implant demonstrated its intended position over the jaw angle.
A plastic model of the custom jaw angle implant demonstrated its intended position over the jaw angle.


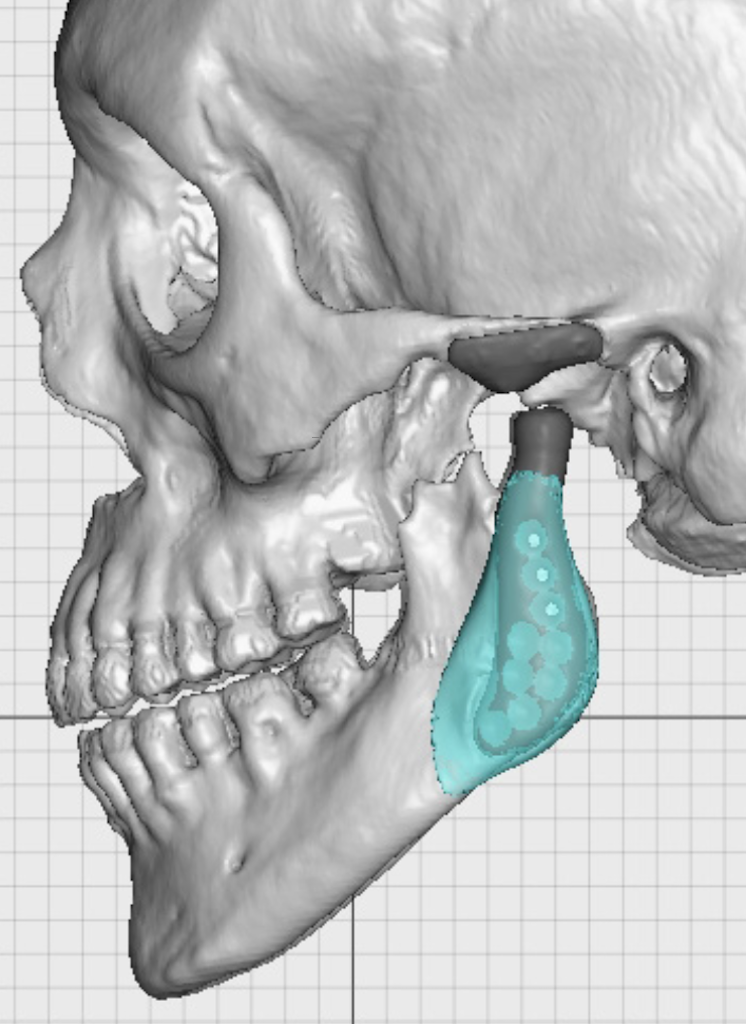
 Through the preauricular incision, the titanium ramus component of the TMJ prosthesis was exposed at the deep subperiosteal level, and the implant pocket was created. The custom jaw angle implant was passed through the incision, positioned over the metal plate, and secured with a single screw engaging the portion of the implant resting on native bone. The implant pocket was then closed over the device.
Through the preauricular incision, the titanium ramus component of the TMJ prosthesis was exposed at the deep subperiosteal level, and the implant pocket was created. The custom jaw angle implant was passed through the incision, positioned over the metal plate, and secured with a single screw engaging the portion of the implant resting on native bone. The implant pocket was then closed over the device.
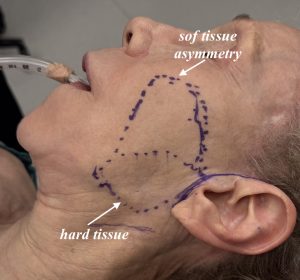
 A separate anterior skin flap was elevated in the subcutaneous plane over the area of soft-tissue deficiency. Medium-thickness AlloDerm grafts measuring 2 × 8 cm were placed beneath the skin flap, corresponding to the areas of external asymmetry identified preoperatively.
A separate anterior skin flap was elevated in the subcutaneous plane over the area of soft-tissue deficiency. Medium-thickness AlloDerm grafts measuring 2 × 8 cm were placed beneath the skin flap, corresponding to the areas of external asymmetry identified preoperatively.
 The incision was closed with resorbable sutures, completing the composite facial asymmetry correction.
The incision was closed with resorbable sutures, completing the composite facial asymmetry correction.
Discussion
Facial asymmetry commonly consists of both hard- and soft-tissue components, each requiring a different corrective strategy, even when addressed during the same operation. The hard-tissue component can be accurately quantified using three-dimensional CT imaging. The presence of hardware in the jaw angle region does not preclude the design or placement of custom implants, and a TMJ prosthesis does not pose additional challenges in this regard.
The soft-tissue component of facial asymmetry is determined primarily by clinical assessment and estimation of the volume deficit. Although fat grafting remains the most common and versatile method of soft-tissue augmentation, retention rates in thin, older patients are often poor. In such cases, dermal grafts placed through facelift-type incisions and flaps provide a more reliable and sustained, albeit modest, augmentation effect.
Key Points
- Total TMJ replacement provides significant functional improvement but does not correct existing facial asymmetry and may accentuate it.
- Custom jaw angle implants can be designed to overlay the ramus component of a TMJ prosthesis to correct structural asymmetry.
- Soft-tissue facial asymmetry can be effectively augmented with allogeneic dermal grafts when fat grafting has failed.
- By combining a custom jaw implant with soft-tissue support, facial asymmetry after TMJ replacement can be safely and predictably improved.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon