

The zygomatic arch is a critical structural and aesthetic component of the midface. While commonly discussed in relation to cheek augmentation, its role is distinct from that of the malar eminence. The arch primarily influences facial width, lateral contour, and overall skeletal balance rather than anterior projection.
Anatomically, the zygomatic arch is formed by the bony junction between the zygomatic and temporal bones. This thin osseous bridge allows passage of the temporalis muscle to its mandibular insertion and contributes significantly to the lateral cheek contour. Although it serves as an origin for the masseter muscle, the arch itself is a fixed structure and does not directly participate in mastication.
Traditional cheek augmentation addresses two complementary regions: the malar eminence (anterior cheek) and the zygomatic arch (lateral cheek). While malar implants are widely recognized, isolated augmentation of the zygomatic arch remains less commonly discussed. Zygomatic arch implants represent a distinct implant category designed specifically to enhance lateral cheek width and definition without increasing anterior cheek volume.
Definition and Design Characteristics
 Isolated zygomatic arch implants are engineered to augment the lateral cheekbone exclusively. Their defining features include posterior and lateral positioning relative to the malar eminence, absence of anterior cheek fullness, and selective enhancement of the outer cheek contour. The aesthetic effect emphasizes skeletal strength and angularity rather than cheek roundness or youthful fullness. These implants are particularly visible in oblique and profile views, where lateral cheek sweep contributes significantly to facial structure.
Isolated zygomatic arch implants are engineered to augment the lateral cheekbone exclusively. Their defining features include posterior and lateral positioning relative to the malar eminence, absence of anterior cheek fullness, and selective enhancement of the outer cheek contour. The aesthetic effect emphasizes skeletal strength and angularity rather than cheek roundness or youthful fullness. These implants are particularly visible in oblique and profile views, where lateral cheek sweep contributes significantly to facial structure.
Aesthetic Indications
Patients most suitable for isolated zygomatic arch augmentation typically demonstrate adequate anterior malar projection but insufficient midfacial width. Common indications include the desire for sharper, more angular cheekbones; a masculine or athletic facial contour; correction of arch flattening due to aging, trauma, or congenital deficiency; and restoration of lateral facial balance in patients with a wide lower face or mandibular implants.
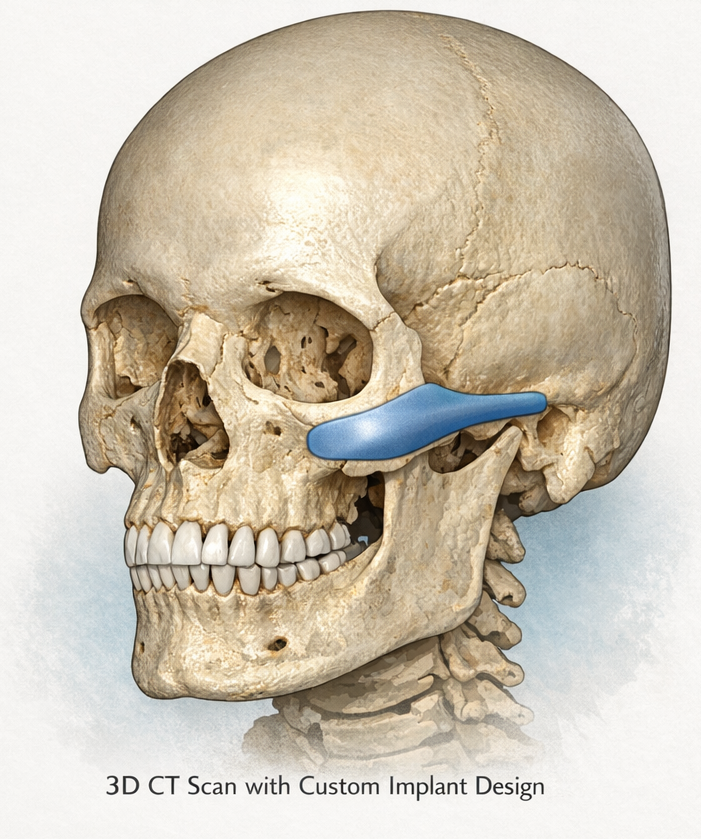
Custom Implant Design
 Due to historically low demand, standardized zygomatic arch implants do not exist. Consequently, custom-designed implants are the only reliable method for isolated arch augmentation. Effective implant design must precisely replicate the curvature of the zygomatic arch, allow controlled lateral width enhancement, taper smoothly toward the temporal bone, and include an anterior extension to facilitate placement and provide a site for screw fixation. These design elements are critical to achieving predictable aesthetic outcomes and stable fixation.
Due to historically low demand, standardized zygomatic arch implants do not exist. Consequently, custom-designed implants are the only reliable method for isolated arch augmentation. Effective implant design must precisely replicate the curvature of the zygomatic arch, allow controlled lateral width enhancement, taper smoothly toward the temporal bone, and include an anterior extension to facilitate placement and provide a site for screw fixation. These design elements are critical to achieving predictable aesthetic outcomes and stable fixation.
Surgical Considerations
Zygomatic arch implants are typically placed through an intraoral approach with careful subperiosteal dissection confined to the narrow contours of the arch. Special attention is required to protect the zygomaticotemporal nerve as it crosses the posterior arch. Given the superficial visibility of this region, millimeter-level accuracy in implant size selection and positioning is essential to avoid contour irregularities or asymmetry.
Comparison With Standard Cheek Implants
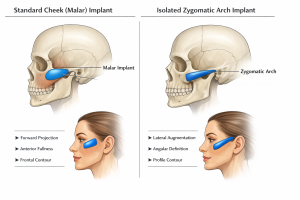 Standard cheek implants primarily enhance forward projection at the malar eminence and are most impactful in frontal facial views, producing fullness and a youthful appearance. In contrast, isolated zygomatic arch implants increase lateral facial width and definition, with their greatest aesthetic impact observed in oblique and profile views. Rather than fullness, they emphasize structural strength and skeletal definition.
Standard cheek implants primarily enhance forward projection at the malar eminence and are most impactful in frontal facial views, producing fullness and a youthful appearance. In contrast, isolated zygomatic arch implants increase lateral facial width and definition, with their greatest aesthetic impact observed in oblique and profile views. Rather than fullness, they emphasize structural strength and skeletal definition.
Conclusion
Isolated zygomatic arch implants provide a highly selective method for enhancing lateral cheekbone width and definition without altering anterior cheek projection. When designed as custom implants and placed with precision, they offer a powerful yet controlled approach to improving midfacial balance and skeletal contour, particularly in patients who do not require traditional malar augmentation.
Barry Eppley, MD
World-Renowned Plastic Surgeon