

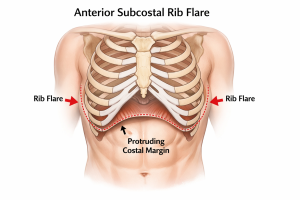
 Subcostal rib flare refers to the outward protrusion of the lower ribs, most commonly ribs 8–12, at the lower costal margin. It is primarily an osteocartilaginous issue, not a soft-tissue problem.
Subcostal rib flare refers to the outward protrusion of the lower ribs, most commonly ribs 8–12, at the lower costal margin. It is primarily an osteocartilaginous issue, not a soft-tissue problem.
Its key characteristics include:
- Visible outward angulation of the lower rib cage
- Most noticeable from:
- Frontal view (V-shaped or squared costal margin)
- Oblique view (ribs “kick out” anteriorly)
- Often asymmetric
- Becomes more apparent in lean patients
While does affect the entire lower ribcage to some degree it is most commonly seen as an anterior protrusion more so than a lateral or widening protrusion.
Effective treatment of subcostal rib flare is surgical in nature. The traditional approaches are either costal contouring (rib cartilage shaving), rib resection or a combination of both. While effective they require an incision along the lateral subcostal margin which is not in a natural skin crease and is visible. As a result percutaneous and limited incision approaches have been described each with their advocates…but with limited long term data of their effectiveness, stability and safety profile.
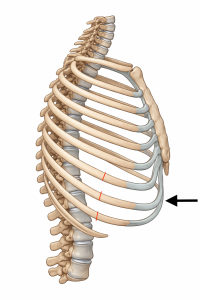
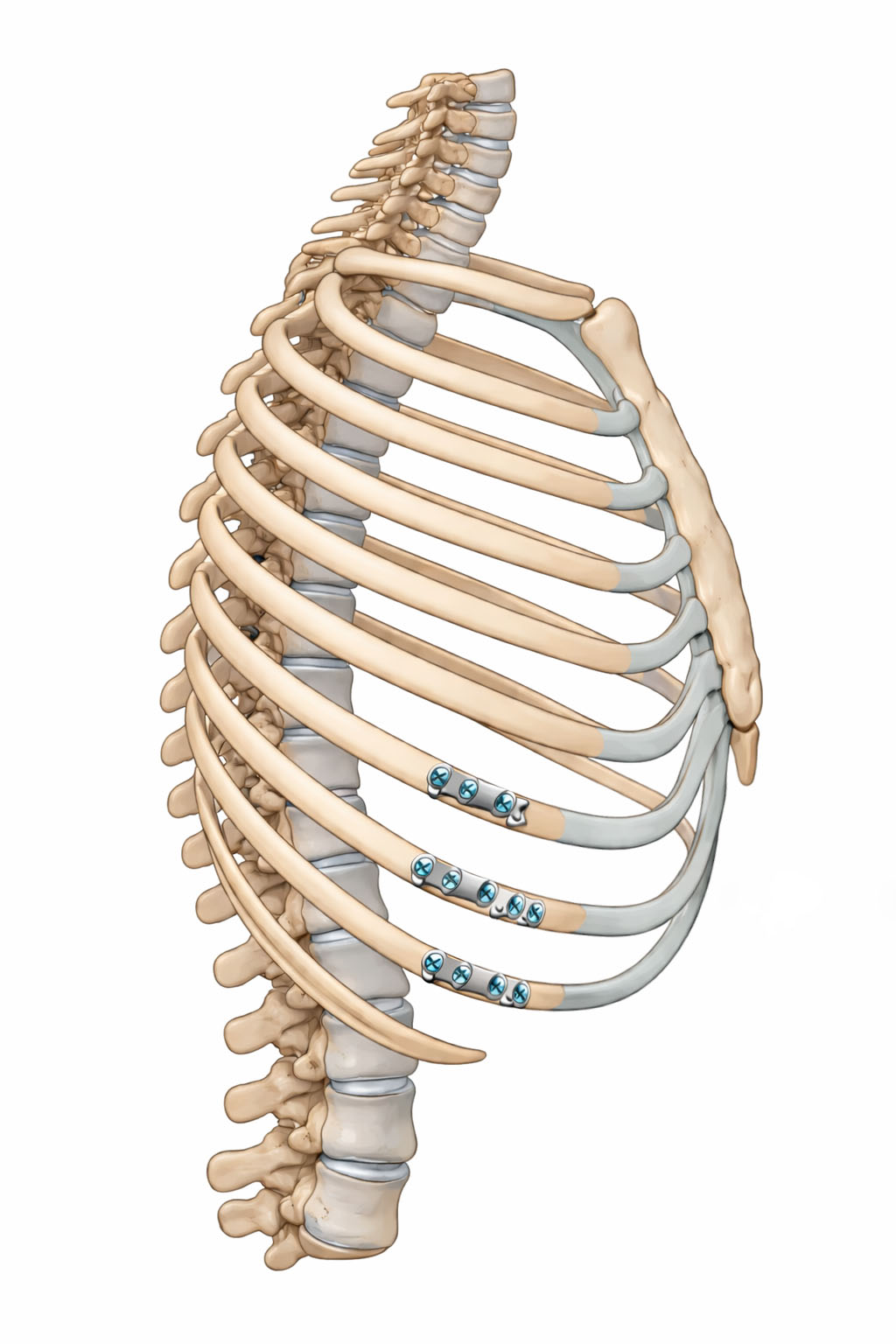
 One of the limited incisional techniques is lateral osteotomies of ribs 6, 7 and 8 to create a greenstick fracture. With compression at the medial lower subcostal ribcage this allows the medial rib bone at the fracture line to be bent inward and a plate applied to hold it which reduces the amount of anterior subcostal rib flare. In essence this is a ribcage remodeling technique based on an osteosythesis rib bending method. The goal is to reduce anterior rib projection and chest width, not to remove ribs entirely.
One of the limited incisional techniques is lateral osteotomies of ribs 6, 7 and 8 to create a greenstick fracture. With compression at the medial lower subcostal ribcage this allows the medial rib bone at the fracture line to be bent inward and a plate applied to hold it which reduces the amount of anterior subcostal rib flare. In essence this is a ribcage remodeling technique based on an osteosythesis rib bending method. The goal is to reduce anterior rib projection and chest width, not to remove ribs entirely.
This procedure has become known by the acronym of ARCO or anterior ribcage osteotomy. It is typically considered for patients with:
- Wide or protrusive lower rib cage
- Barrel-shaped anterior chest
- Rib flare that does not respond to physical therapy or external compression treatments
- Desire for a narrower waist–chest transition in aesthetic body contouring cases
How ARCO Differs From Rib Resection
|
ARCO |
Rib Resection |
|
Rib reshaping |
Rib removal |
|
Employs rib fracture bending |
Remaining subcostal ribcage remains stable |
|
Requires fracture healing |
Soft tissue healing only |
|
Plate fixation required |
No hardware needed |
Risks & Considerations
Like all ribcage procedures ARCO has potential complications including:
- Pneumothorax
- Chest wall instability
- Chronic pain or intercostal nerve injury
- Asymmetry
- Nonunion or malunion of rib segments
- Respiratory compromise if over-corrected
To date based on limited case series reports of such postoperative complications have not been seen to occur.
Recovery
- Significant postoperative pain (ribs are involved)
- Activity restriction for 6–8 weeks
- Full skeletal stabilization may take 3–4 months
- Compression garments or external support is required
The reduction of the prominence of a subcostal rib flare by lateral osteotomies, which creates a bend in the ribs , works by the flexibility of the cartilaginous portion of the lower subcostal ribs. Banding or postoperative compression across the lower costal ribcage is still needed. But the purpose of the banding is to support the rib reshaping as it heals and is not solely responsible for the effect.
Dr. Barry Eppley
World-Renowned Plastic Surgeon